Peroxphos
Member
- Joined
- Dec 15, 2019
- Messages
- 59
What thiamine dose solved your issues?suggested reading:
"There are indications that a thiamine deficiency heightens susceptibility to mercury toxicity. Many of the symptoms of mercury poisoning are observed in persons with thiamine deficiency."
An Artist's Decades Long Dysautonomia Treated With Thiamine - Hormones Matter
Here is the story of my longstanding thiamine deficiency, which was not recognized by doctors.www.hormonesmatter.com
also this article: Detoxing From Heavy Metals
"Mercury Toxicity: Depletes glutathione (an incredible antioxidant that regenerates itself in the liver. It’s one of the important molecules you need to stay healthy and prevent disease."
I've been living with mercury poisoning and lead poisoning for many years. I've been taking high dose thiamine hcl for about 18 months. It has brought my glutathione level back up to normal. My glutathione level was very low for many years. Thiamine hcl chemically bonds to lead (making the bonded thiamine unavailable to the body) and lead poisoning symptoms and thiamine deficiency symptoms are identical. I no longer have lead poisoning symptoms.
also:
Thiamine deficiency and nervous system function disturbances - PubMed
Thiamine is important for oxidative metabolism, and B1 deficiency is thought to give rise to polyneuropathies. A group of male Wistar rats (n = 15) received a vitamin B1 deficient diet (group-a), and the pair fed control group (n = 20, group-b) received a normal diet with no vitamin deficiency...pubmed.ncbi.nlm.nih.gov
How Can Something As Simple as Thiamine Cause So Many Problems? - Hormones Matter
Is thiamine deficiency too simple to explain the devastating nature of the systemic adverse reactions to some vaccines and medications?
Thiamine lowers brain serotonin:
also:Effect of thiamine deficiency on brain serotonin turnover - PubMed
Serotonin turnover has been investigated in regional brain areas of rats made thiamine deficient by pyrithiamine (PT). Following intracisternal injection of [14C]5-hydroxytryptamine ([14C]5-HT), a marked increase in the accumulation of [14C]5-hydroxyindoleacetic acid ([14C]5-HIAA) was found in...
Serotonin Syndrome and Thiamine: Is There a Connection? - Hormones Matter
A mild deficiency of thiamine is responsible for the large number of the polysymptomatic illnesses reported.
I've found a lot more benefit from thiamine supplementation than from cypro. Cypro tends to cause constipation. Thiamine hcl normalized my entire digestive tract.
also: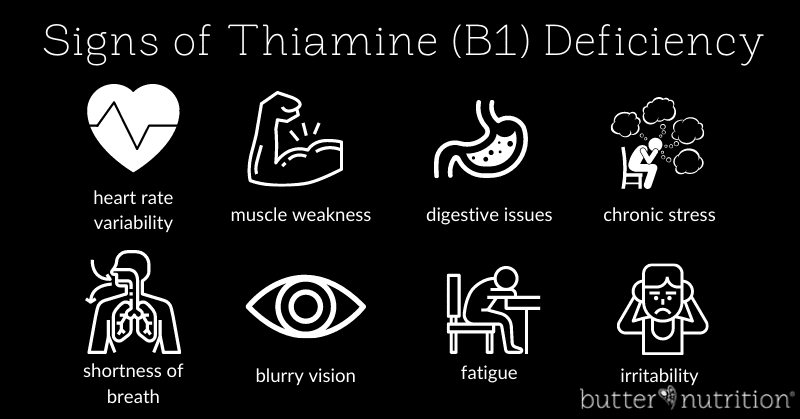
13 Signs of Thiamine Deficiency (B1)
Cliff notes: Thiamine deficiency was not solved decades ago by enriching grains and is alive and well. The implications of this have a huge impact on modern day health and disease. It's always been amazing to me that a country with an endless food supply and resources can coexist with so much...butternutrition.com
"In the early stages of beriberi the ANS is unbalanced, so that either the sympathetic or parasympathetic, normally working in synchrony, dominates the reaction, adversely affecting blood pressure, pulse rate and many other adaptive mechanisms, like POTS. It can be seen that the patient with POTS or beriberi is essentially maladapted and is unable to adjust bodily systems to meet environmental changes. Edema (swelling in parts of the body), a cardinal feature of beriberi, supported a diagnosis of thiamine deficiency in this mother’s daughter. Also, Gardasil is a yeast vaccine and an enzyme called thiaminase, whose action destroys thiamine, is known to be in the yeast. Thiaminase disease has been reported in Japan in association with dietary thiamine deficiency."
Post Gardasil POTS and Thiamine Deficiency- Hormones Matter
Postural Orthostatic Tachycardia Syndrome (POTS) observed post gardasil with a critical link to thiamine deficiency.
The Sugar - Thiamine Connection in Adverse Reactions
Diets high in sugar may contribute to thiamine deficiency and vaccine or medication induced autonomic dysregulation - an emerging hypothesis.
Are we talking standard high dose 100-300mg daily or megadose 1-2g daily?