I think the conversion to DHT is what matters rather than the T level itself. I doubt serum DHT levels correlate with tissue levels as T locally converts to DHT in cells and tissues. Besides the benefits is actually from how much to T,DHT is binding to cell(say AR) rather than the serum levels itself. Tubzy once took an AR receptor antagonist, his T and E2 levels were same but got massive estrogenic effectsI'm not a fan of TRT. It converts into estrogen too easily. And moreover, the CAUSE of low T isn't addressed when you just take TRT. If you fix the metabolic underlying issues, testosterone can easily double or triple. I think it is a really bad way to go until you've figured out what is causing low T and tried to fix it.
Same as for instance taking insulin. I would fix diabetes in any way possible, if I had type 2, without resorting to insulin.
I've found that men taking T always experience issues with it. And some are quite serious.
Also, the fact is there are many men throughout the world who function just fine, and are perfectly masculine, with T that is more like 300 or so.
Testosterone levels among Aché hunter-gatherer men : A functional interpretation of population variation among adult males. - PubMed - NCBI
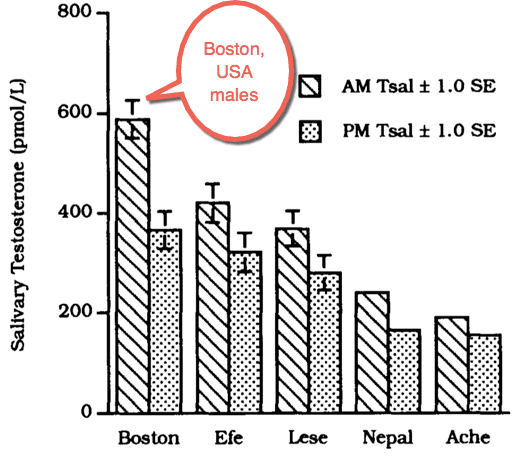
Salivary testosterone levels were measured in a population of New World indigenous adult hunter-gatherer males in order to compare circulating levels of free unbound bioactive steroid with those previously reported among Boston and nonwestern males.
The study population consisted of adult Aché hunter-gatherer males (n=45) living in eastern Paraguay.
Morning and evening salivary testosterone levels (TsalA.M.; TsalP.M.) among the Aché were considerably lower than western values (Boston) and even lower than other previously reported nonwestern populations (Efe, Lese, Nepalese).
No association was observed between height, weight, or age and salivary testosterone levels within the Aché group, although older men (ages>40) were poorly represented in the study sample.
Nevertheless, a mild correlation was observed between Aché Tsal A.M. levels and BMI (r=0.133,p=0.0725).
Comparison of Aché values with those for other populations confirms the prevalence of significant interpopulational variation in testosterone levels among adult males.
Interpopulational variation in male testosterone is not as great, however, as has been documented for ovarian steroids among females, nor is it likely that such variation reflects differences in male fecundity.
Nevertheless, such interpopulational variation in salivary testosterone levels may have a functional significance in the regulation of protein anabolism in skeletal muscle, thereby affecting the overall energy budget of the organism. It is suggested that relative suppression of average testosterone may be adaptive under conditions of chronic energy shortage.
-----
Here is a comparison. Now admittedly, these Ache men may have parasites and bugs, but on the other hand they are physically active and may have some advantages over those living in, say, Boston:
-
By using this site you agree to the terms, rules, and privacy policy.
-
Charlie's Restoration Giveaway #2 (Entire Home EMF Mitigation & Protection Along With Personal Protection) - Click Here To Enter
-
Dear Carnivore Dieters, A Muscle Meat Only Diet is Extremely Healing Because it is a Low "vitamin A" Diet. This is Why it Works so Well...
Rest the rest of this post by clicking here
-
The Forum is transitioning to a subscription-based membership model - Click Here To Read
Click Here if you want to upgrade your account
If you were able to post but cannot do so now, send an email to admin at raypeatforum dot com and include your username and we will fix that right up for you.
Testosterone
- Thread starter Syncopated
- Start date

EMF Mitigation - Flush Niacin - Big 5 Minerals