michael94
Member
- Joined
- Oct 11, 2015
- Messages
- 2,419
I was writing a response to gbolduev's post here: IP6 For Iron Chelation My response was getting a bit long and unrelated to IP6 so I just decided to make a new thread.
1. Xanthine Oxidase
Let's start with xanthine oxidase. I was doing research and it seems like xanthine dehydrogenase is the enzyme for exporting non-heme iron. There are three xanthine oxioreductase forms and xanthine oxidase is generally the most problematic unless tightly controlled but I won't get too much into those details because it's beyond my chemistry/biology abilities. Suffice it to say all of them play an important role in the body and it's probably inaccurate to say xanthine oxidase is "bad". Both XDH and XO are inhibited by nitric oxide and in addition the radical formation associated with XO is greatly attenuated by methyelene blue. Alcohol inhibits XDH too so we can start to see the connection between alcohol liver damage and iron accumulation. This obviously points to the benefits of MB as a therapeutic agent along raising the NAD/NADH in general. Of course MB acts in more ways than just restoring XDH activity but that's definitely one of the main mechanisms. Google MB + liver damage and see for yourself. I really doubt molybdenum/B2 levels are the limiting factors in people not eating weird super-restrictive diets although that may be wrong, open to being convinced otherwise.
2. Low Estrogen
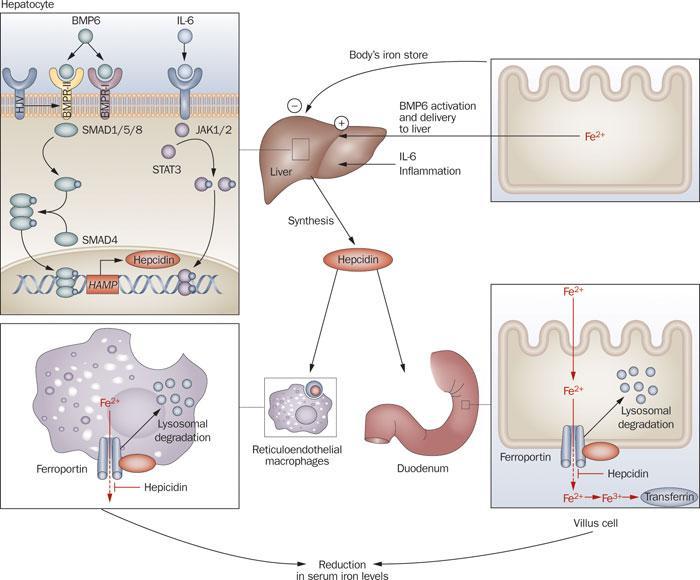
Gbolduev covered everything on that issue pretty well. Low estrogen lowers ceruloplasmin as well as raises hepcidin which blocks the export of iron from the liver, see image below. Low vitamin D and inflammation in general also raises hepcidin.
This is all a very individual thing.Some people have high estrogen or normal estrogen and may still have iron metabolism problems but in people with too low estrogen it IS contributing to the problem no doubt about it. Pregnenolone/DHEA supplementation may be in order because low pregnenolone/DHEA/Estrogen etc can be a vicious cycle to get out of especially if you have gut problems. Temporary raising of steroids back to healthy levels can re-allow the egress of unnecessary non-heme iron and excess copper and lead to good long term endogenous production by reducing excess iron and copper related oxidative stress. If zinc is not being utilized properly due to low estrogen then you are fighting an uphill battle against poor liver function. Zinc is necessary for vitamin A to work and both contribute to the breakdown of fibrotic tissue. That stuff won't show up in your liver ALT/AST levels and your clown doctor will say liver is fine. Dipshits. Pregnenolone itself also has important anti-fibrotic actions. I know @haidut mentioned pregnenolone alone having a important role in liver toxin management so there's another benefit although I had a hard time finding info on that specifically.
3. L-Carnitine
L-carnitine is very important, thanks to @kineticz for turning me onto this substance. In my experience it has a very good stabilizing effect on energy levels and blood flow. I could write a lot but I'll just spam some studies and you can come to your own conclusions.
- Neuroprotective Effects of Pre-Treament with l-Carnitine and Acetyl-l-Carnitine on Ischemic Injury In Vivo and In Vitro -----> Role of xanthine oxidase in ischemia/reperfusion injury. - PubMed - NCBI ( tying back into XO/XDH connection )
- Plasma carnitine concentrations after chronic alcohol intoxication. - PubMed - NCBI
- https://sci-hub.io/10.1016/0024-3205(96)00343-8
- L-carnitine ameliorated fatty liver in high-calorie diet/STZ-induced type 2 diabetic mice by improving mitochondrial function
- L-Carnitine Prevents Progression of Non-Alcoholic Steatohepatitis in a Mouse Model with Upregulation of Mitochondrial Pathway
- L-carnitine ameliorated fasting-induced fatigue, hunger, and metabolic abnormalities in patients with metabolic syndrome: a randomized controlled study
- Effect of acetyl-L-carnitine on lipid peroxidation and xanthine oxidase activity in rat skeletal muscle. - PubMed - NCBI
inb4 carnitine lowers thyroid, discussed on this page: PUFA Depletion Can (probably) Be Accomplished In 30 Days!
Retention of iron in the liver is due to low estrogen. Peat is super wrong on this. Women after menopause start retaining iron in their livers also, since their estrogen levels fall.
Basically if you are stressed you will use a lot of pregnenolone to make progesterone for cortisol and aldo pathway and will have very little DHEA. That will put your testosterone and estradiol into the lower part of the range. And you will start accumulating iron and copper in the liver. The mechanism how it works is this.
To release iron from the liver you need xanthine oxidase which runs on vitamin B2 and molybdenum, then you need ceruloplasmin to oxidize iron and put it on transferrin.
SO here we can possibly have 2 problems , lack of B2 or molybdenum , and lack of DHEA from stress so there is very little estrogen made.LOW estrogen equals low ceruloplasmin which equals no iron on transferrin and tons of it in ferritin.
Another problem is suppressing estrogen)))) like Peat advices, and then you run low on zinc no matter what you do and you wear glasses as thick as a windshield in your car)). Estrogen is needed to make zinc bioavailable since without bioavailable copper that estrogen provides your zinc levels will be suppressed. And when you run low on bioavailable zinc your protein synthesis goes down the drain and what suffers first. Yes you got it, the tiny muscles around your eyes. NOW we look at the thickness of PEATs glasses))) Cant see his eyes behind those. It is funny that I had exactly the same when I got sick before I got into all this medical crap. I remember I was driving a car and I could not see the signs on the road and my eyes constantly got tired .
SO the good idea would be to test your DHEA,Pregnenolone and also B2 and molybdenum status. IF you have low pregnenolone, that is most likely you have SIBO in the gut, since prenenolone is made from cholesterol and koenzym A which requires B5 in its active form --pantethine and acetic acid( vinegar).
B5 recycling depends on the gut.
That is why so many people are helped with simple vinegar plus brewest yeast.
Also iron chelation is good, but dont forget we have low iron in tissues but some free iron in the organs and also tons of iron in the liver. SO I think proper iron chelation would be by making iron bioavailable so it does not spill from the liver and making sure you have proper ceruloplasmin levels to make iron work.
I hope this makes sense
Serum estradiol associates with blood hemoglobin in elderly men: the MrOS Sweden study. - PubMed - NCBI
Estrogen regulates iron homeostasis through governing hepatic hepcidin expression via an estrogen response element. - PubMed - NCBI
I usually dont look at these, but the first study was Swedish , so may be not as bull**** as FDA controlled crap on pubmed)))
1. Xanthine Oxidase
Let's start with xanthine oxidase. I was doing research and it seems like xanthine dehydrogenase is the enzyme for exporting non-heme iron. There are three xanthine oxioreductase forms and xanthine oxidase is generally the most problematic unless tightly controlled but I won't get too much into those details because it's beyond my chemistry/biology abilities. Suffice it to say all of them play an important role in the body and it's probably inaccurate to say xanthine oxidase is "bad". Both XDH and XO are inhibited by nitric oxide and in addition the radical formation associated with XO is greatly attenuated by methyelene blue. Alcohol inhibits XDH too so we can start to see the connection between alcohol liver damage and iron accumulation. This obviously points to the benefits of MB as a therapeutic agent along raising the NAD/NADH in general. Of course MB acts in more ways than just restoring XDH activity but that's definitely one of the main mechanisms. Google MB + liver damage and see for yourself. I really doubt molybdenum/B2 levels are the limiting factors in people not eating weird super-restrictive diets although that may be wrong, open to being convinced otherwise.
2. Low Estrogen
Gbolduev covered everything on that issue pretty well. Low estrogen lowers ceruloplasmin as well as raises hepcidin which blocks the export of iron from the liver, see image below. Low vitamin D and inflammation in general also raises hepcidin.
This is all a very individual thing.Some people have high estrogen or normal estrogen and may still have iron metabolism problems but in people with too low estrogen it IS contributing to the problem no doubt about it. Pregnenolone/DHEA supplementation may be in order because low pregnenolone/DHEA/Estrogen etc can be a vicious cycle to get out of especially if you have gut problems. Temporary raising of steroids back to healthy levels can re-allow the egress of unnecessary non-heme iron and excess copper and lead to good long term endogenous production by reducing excess iron and copper related oxidative stress. If zinc is not being utilized properly due to low estrogen then you are fighting an uphill battle against poor liver function. Zinc is necessary for vitamin A to work and both contribute to the breakdown of fibrotic tissue. That stuff won't show up in your liver ALT/AST levels and your clown doctor will say liver is fine. Dipshits. Pregnenolone itself also has important anti-fibrotic actions. I know @haidut mentioned pregnenolone alone having a important role in liver toxin management so there's another benefit although I had a hard time finding info on that specifically.
3. L-Carnitine
L-carnitine is very important, thanks to @kineticz for turning me onto this substance. In my experience it has a very good stabilizing effect on energy levels and blood flow. I could write a lot but I'll just spam some studies and you can come to your own conclusions.
- Neuroprotective Effects of Pre-Treament with l-Carnitine and Acetyl-l-Carnitine on Ischemic Injury In Vivo and In Vitro -----> Role of xanthine oxidase in ischemia/reperfusion injury. - PubMed - NCBI ( tying back into XO/XDH connection )
- Plasma carnitine concentrations after chronic alcohol intoxication. - PubMed - NCBI
- https://sci-hub.io/10.1016/0024-3205(96)00343-8
- L-carnitine ameliorated fatty liver in high-calorie diet/STZ-induced type 2 diabetic mice by improving mitochondrial function
- L-Carnitine Prevents Progression of Non-Alcoholic Steatohepatitis in a Mouse Model with Upregulation of Mitochondrial Pathway
- L-carnitine ameliorated fasting-induced fatigue, hunger, and metabolic abnormalities in patients with metabolic syndrome: a randomized controlled study
- Effect of acetyl-L-carnitine on lipid peroxidation and xanthine oxidase activity in rat skeletal muscle. - PubMed - NCBI
inb4 carnitine lowers thyroid, discussed on this page: PUFA Depletion Can (probably) Be Accomplished In 30 Days!