A systems-approach to NAD+ restoration
A decline in NAD+ is a feature of ageing and may play a causal role in the process. NAD+ plays a pivotal role in myriad processes important in cellula…
Alternative strategies to boost NAD+
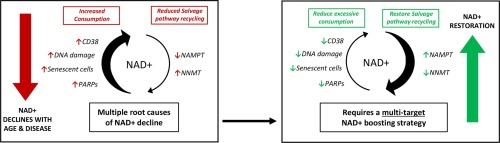
Given these drawbacks of simple precursor supplementation, strategies that address the root causes of NAD+ decline by considering multiple key nodes of the NAD+ interactome seem more appealing. Furthermore, there is already a wealth of evidence to support these targets as interventions.Targeting hyperactivated NAD+ consumption
CD38 inhibition
CD38 inhibition has emerged as a promising strategy to increase cellular NAD+ . Given the inefficient use of NAD+ by CD38, strategies to inhibit CD38 even at a low level may lead to substantial increases in cellular NAD+ levels. In support of this, CD38 inhibition by the flavonoid apigenin resulted in a 50% increase in NAD+ [106], [107], which is comparable with reported NAD+ increases using 300 mg NR (Table 1). This intervention was also found to decrease global proteome acetylation and improve glucose and lipid homeostasis in obese mice by increasing the activity of downstream SIRT1 and SIRT3 [81], [106]. The CD38 inhibitor 78c has also been found to reverse age-related NAD+ decline and improve several physiological and metabolic parameters of ageing, including glucose tolerance, muscle function, exercise capacity and cardiac function in mouse models of natural and accelerated ageing [82]. In addition, aged wild-type mice were shown to have around half the NAD+ levels of young mice, whilst CD38 knockout mice maintained their NAD+ levels and were resistant to the negative effects of a high fat diet, including liver steatosis and glucose intolerance, adding further support to CD38 inhibition being an attractive approach [23], [82], [106].PARP inhibition
The detrimental action of PARP activity on NAD+ pools is evident in experiments where cells are treated with genotoxic agents to promote DNA damage. These agents lead to a sustained activation of PARP activity and a concomitant decrease in NAD+ levels to only 10–20% of their normal levels within 5–15 min [108], [109]. Studies in DNA repair-deficient human neuroblastoma cells have shown that treatment with PARP inhibitors can reduce DNA-damage associated NAD+ loss [71]. In mouse models of early alcoholic steatohepatitis, a condition associated with NAD+ decline, pharmacological inhibition of PARP with Olaparib restored the hepatic NAD+ content and beneficially affected metabolic, inflammatory and oxidative stress parameters via increased SIRT1 activation [27], [110]. Congruently, in PARP1 KO mice NAD+ levels were robustly increased in brown adipose tissue (BAT) and skeletal muscle by approximately 100% and 50% respectively, improving mitochondrial function [24], [111]. PARP inhibitors have also proved promising in models of Cockayne Syndrome (CS) and Xeroderma Pigmentosum (XDP), accelerated ageing disorders characterised by persistent PARP activation and NAD+ decline. Notably, treatment of CS mice with PARP1 inhibitors promoted lifespan extension and ameliorated the severe phenotypes caused by PARP1 hyperactivation [11], [70].Targeting NAD+ salvage and recycling
NAMPT activation
Studies to reverse the age-related decline in the Salvage pathway by activating its rate-limiting enzyme NAMPT have also yielded promising results with regard to increasing NAD+ levels. Overexpression of NAMPT in mice was found to increase intracellular NAD+ levels in skeletal muscle by ∼50%, an increase comparable with the effects of dietary NAD+ precursors (Table 1) [112]. The potential of NAMPT to restore NAD+ has also led to the development of small molecule activators. The aminopropyl carbazole P7C3 was able to rescue human cells in vitro from doxorubicin-induced NAD+ depletion [113], whilst in vivo P7C3 administration to mice increased brain NAD+ levels and offered protection from ischemic stroke [113], [114]. SBI-797812, another small molecule activator of NAMPT, increased NAMPT activity and NAD+ levels in a dose dependent manner elevating NAD+ by ∼40% in mouse liver [115]. The tripeptide Ile-Arg-Trp (IRW) has also recently been found to increase both NAMPT and NAD+ levels in muscle cells of obese mice [116]. Aside from the influence of pharmacological interventions, NAMPT levels fluctuate to match cellular NAD+ demand and as a result are influenced by activities that effect cellular energy stress such as fasting, calorie restriction and exercise [117], [118], [119]. Accordingly, in an exercise intervention study NAMPT protein increased by 127% in sedentary nonobese subjects after only three weeks of exercise training [119]. Another study demonstrated ten weeks of resistance training increased NAMPT levels in the muscle of middle-aged men by 15%, which was associated with a 127% increase in NAD+ levels [9]. This demonstrates that lifestyle interventions may also be a powerful strategy for NAD+ enhancement where clinically appropriate.NNMT inhibition
NNMT was found to be overexpressed in the white adipose tissue (WAT) and liver of obese and diabetic mice, both of which are associated with decreased NAD+ [26], [104]. NNMT knockdown was found to restore NAD+ and SAM indicating that NNMT inhibition promotes recycling of NAM to NAD+ via the Salvage pathway rather than methylation and excretion [26]. Treatment of mouse adipocytes with the NNMT inhibitor 5-amino-1MQ resulted in a concentration-dependent increase in NAD+ levels by ∼1.2–1.6-fold relative to control adipocytes. Elevated SAM was also observed improving the availability of methyl groups to the cell [120]. Furthermore, treating mice with diet-induced obesity with a NNMT inhibitor caused significant loss of body weight and white adipose tissue mass, reduction in adipocyte size and decreased circulating cholesterol levels [120].Designing better NAD+ Supplementation — SOLR
You may be contemplating taking an NAD supplement after feeling some notable changes in your body such as decline in energy levels, decreased strength or stamina in the gym and longer recovery times. There are many options within the NAD supplement world, and we want you to choose the best option wh
 www.solrglobal.com
www.solrglobal.com
Designing better NAD+ Supplementation
It is evident that a multitargeted approach is needed: an NAD+ precursor, promotion of NAD+ synthesis enzymes, suppression of NAD+ destroying enzymes and suppression of NAD+ excretion.- Increasing NAD+ synthesis enzymes: flavonoids such as quercetin, rutin and troxrutin all increase NAMPT to restore the salvage pathway.
- Decreasing wasteful NAD+ consumption: apigenin and quercetin are both CD38 inhibitors.
- Decreasing NAD+ excretion: EGCG inhibits NMNT and methylation of nicotinamide.