Worth posting this in its own thread,
copper looks to be highly significant in schizophrenia,
where blood levels tend to be higher than normal BUT brain levels lower in copper regardless (due to defective copper transport)
so problem is with transport typically instead of levels, leading to functional deficiency in some brain areas at least:
ATP7A and B, and CTR1 is involved in copper transport
insightful studies
people with schizophrenia not on medication have much lower n-terminus ATP7A expression. much lower transmembrane CTR1 expression. lower ATP7b expression.

and less copper in the substantia nigra brain area tested for copper content
[So this suggests another likely helpful area of focus is finding stuff that increases ATP7a and especially CTR1 expression]
2 basic things,
Vitamin A could help increase atp7a and vitamin D could help increase ctr1 (but need to be balanced)
Interestingly there's been some mention of how schizophrenia has some commonalities with vitamin a excess or deficiency
(i) neurological congenital abnormalities reported in some schizophrenia cases are comparable to those observed with vitamin A deficiency or altered at-RA
(probably either deficiency or excess because like ive mentioned in another post, overload could take away from vitamin D making CTR1 expression worse, where deficiency = not enough ATP7a)
https://www.nature.com/articles/s41380-019-0566-2#Sec7
intake of beta-carotene was demonstrated to be low in some schizophrenia cohorts
https://pubmed.ncbi.nlm.nih.gov/24434091/
^ here a synthetic vitamin a drug was used with positive effect in people with schizophrenia
too much vitamin A could skew things away from CTR1 more by countering vitamin D maybe. so personally i would like a closer ratio of vit D to A than normal. maybe even 1:1 idk its guess work. beef liver is good source of vitamin A + copper but dont want too much
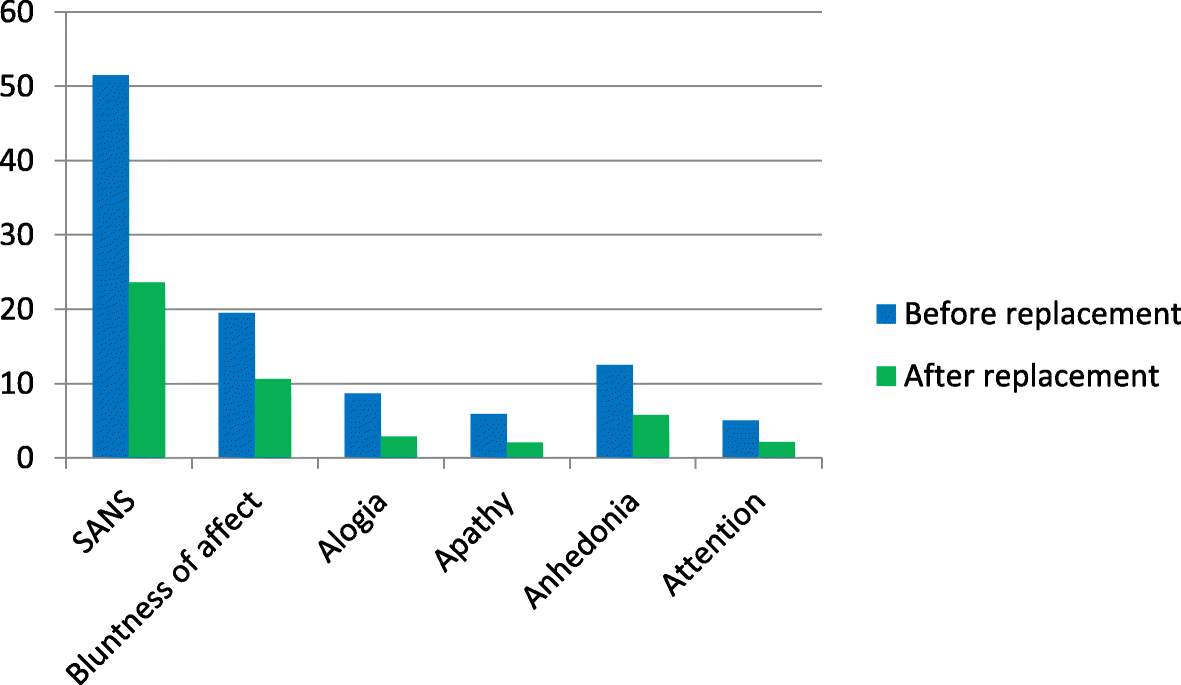
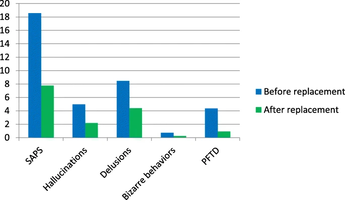
here's vitamin D effect in schizophrenia
 bmcpsychiatry.biomedcentral.com
bmcpsychiatry.biomedcentral.com
(interestingly only 3.8% of people tested had vit d in normal range even though it was summer)
 <---- before & after vitamin D intake for 8 weeks. impressive effect size
<---- before & after vitamin D intake for 8 weeks. impressive effect size
copper looks to be highly significant in schizophrenia,
where blood levels tend to be higher than normal BUT brain levels lower in copper regardless (due to defective copper transport)
so problem is with transport typically instead of levels, leading to functional deficiency in some brain areas at least:
ATP7A and B, and CTR1 is involved in copper transport
insightful studies
These results provide the first evidence of disrupted copper transport in schizophrenia SN that appears to result in a copper-deficient state. Furthermore, copper homeostasis may be modulated by specific dysbindin isoforms and antipsychotic treatment.
Interestingly, decreasing copper activity through by inhibiting transporters or administering the copper chelator cuprizone to mice produces demyelination, altered neurotransmitters, and decreased oligodendrocytic protein expression (Gokhale et al. 2015; Gregg et al. 2009; Herring and Konradi 2011). Additionally, reduced copper activity results in schizophrenia-like behavioural impairments, such as deficits in novel object recognition, spatial memory tasks, pre-pulse inhibition, social interaction, and anxiety
Additionally, schizophrenia patients exhibit decreased metallothionein and glutathione, responsible for intracellular copper chaperoning and transport, that are rescued with antipsychotic treatment (Xuan et al. 2015; Do et al. 2000)(Figure 1B)
In addition to those mentioned previously, lack of copper also exacerbates NMDA-mediated excitotoxic cell death in primary hippocampal neurons
Given the excess of copper in the blood of schizophrenia patients and the increasingly mounting evidence of an abnormal or “leaky” BBB in psychosis, we hypothesize that schizophrenia patients exhibit excess blood copper due to faulty copper transport across the blood brain barrier (BBB). This abnormality would result in a copper-deficient brain state and contribute to the cognitive and behavioral deficits observed in schizophrenia. Our results suggest extracellular copper binding and transport into the cell via CTR1 is impaired in schizophrenia, and not rescued with treatment
Copper transport proteins ^ ,when subdivided by medication status, the N-terminus [ATP7a] protein levels were significantly lower in unmedicated patients versus medicated patients (p=0.02) and controls
Analysis of treatment status revealed that C-terminal ATP7A protein levels were significantly increased only in medicated patients versus controls

people with schizophrenia not on medication have much lower n-terminus ATP7A expression. much lower transmembrane CTR1 expression. lower ATP7b expression.
and less copper in the substantia nigra brain area tested for copper content
[So this suggests another likely helpful area of focus is finding stuff that increases ATP7a and especially CTR1 expression]
2 basic things,
Vitamin A could help increase atp7a and vitamin D could help increase ctr1 (but need to be balanced)
Interestingly there's been some mention of how schizophrenia has some commonalities with vitamin a excess or deficiency
(i) neurological congenital abnormalities reported in some schizophrenia cases are comparable to those observed with vitamin A deficiency or altered at-RA
(probably either deficiency or excess because like ive mentioned in another post, overload could take away from vitamin D making CTR1 expression worse, where deficiency = not enough ATP7a)
https://www.nature.com/articles/s41380-019-0566-2#Sec7
intake of beta-carotene was demonstrated to be low in some schizophrenia cohorts
https://pubmed.ncbi.nlm.nih.gov/24434091/
^ here a synthetic vitamin a drug was used with positive effect in people with schizophrenia
too much vitamin A could skew things away from CTR1 more by countering vitamin D maybe. so personally i would like a closer ratio of vit D to A than normal. maybe even 1:1 idk its guess work. beef liver is good source of vitamin A + copper but dont want too much
here's vitamin D effect in schizophrenia
The psychotropic effect of vitamin D supplementation on schizophrenia symptoms - BMC Psychiatry
Background Schizophrenia is a multifactorial disease involving interactions between genetic and environmental factors. Vitamin D has recently been linked to many metabolic diseases and schizophrenia. Vitamin D plays essential roles in the brain in the context of neuroplasticity, neurotransmitter...
bmcpsychiatry.biomedcentral.com
(interestingly only 3.8% of people tested had vit d in normal range even though it was summer)
"Although our study population consisted of outpatients and blood samples were taken between May and July when sunlight is more intense, the rates of low vitamin D levels were found to be high"
-
Our finding of decreased CTR1 in the cells and fibers of the superficial layers of the entorhinal cortex lends is consistent with the importance of copper in myelin integrity and dendritic spine formation, as well as cellular function. Deficits of myelin and associated oligodendrocytes have been well replicated in schizophrenia in several brain regions
Cortical areas exhibit decreased markers of myelin basic protein (a key component of myelin), fewer oligodendrocytes, abnormal oligodendrocyte morphology, oligodendrocyte degeneration, myelin thickness and laminar abnormalities, as well as downregulation of key myelin related genes and proteins in schizophrenia
. Interestingly, application of the copper chelator cuprizone results in massive, albeit reversible, demyelination and oligodendrocyte death. indicating that copper must play a crucial role in myelin and oligodendrocyte function and integrity. If a deficit of cuprinergic signaling and copper content exists in the superficial layers of the entorhinal cortex in schizophrenia as indicated by our finding of decreased CTR1, this could impact white matter integrity in this area.
In contrast to our findings in the superficial layers of the entorhinal cortex, we observed significantly elevated immunolabeling of CTR1 in the molecular layer of the dentate gyrus, consistent with a trending increase of CTR1 mRNA within the middle temporal area
In further support of our suggestion of compensatory upregulation of CTR1 in the molecular layer of the dentate gyrus in response to copper deficit is the observation that the dentate gyrus exhibits deficient signaling in schizophrenia
Taken together, our data suggest dysregulation of copper transport and homeostasis in the hippocampus and entorhinal cortex in schizophrenia that is region and layer specific, a potential mechanism of schizophrenia pathology that was previously unstudied. Deficient copper within the hippocampus could have deleterious effects, including decreased energy metabolism and neuronal signaling, deficits of myelin maintenance and integrity, and an overall pathological modulation of the trisynaptic pathway crucially involved in memory and cortical function
Therefore, further study is needed to assess cellular copper content and transporter status of each layer and cell type of the hippocampus in schizophrenia, as well as replication of the current study. Abnormal copper and other trace metals are becoming increasingly associated with schizophrenia and other forms of psychosis (Bitanihirwe and Cunningham, 2009; Joe et al., 2018; Schoonover et al., 2018) and therefore could provide a new mechanism to be targeted for development of better treatments. For instance, treatments that mimic the functions of CTR1 might enhance copper transport from the blood to the brain parenchyma could be therapeutic.
Attachments
Last edited:

 Maybe to see a benefit from Retinoic acid I should dose it under the tongue, rubbed on the gums or on the skin... and as for copper if you are toxic and deficient at the same time you risk not absorbing where it is needed (spinal cord and fluid ). Even the hypothesis DMSO + copper or Retinol in the cervical area or spine could be more effective. What do you think of these ideas, even in private if you want.
Maybe to see a benefit from Retinoic acid I should dose it under the tongue, rubbed on the gums or on the skin... and as for copper if you are toxic and deficient at the same time you risk not absorbing where it is needed (spinal cord and fluid ). Even the hypothesis DMSO + copper or Retinol in the cervical area or spine could be more effective. What do you think of these ideas, even in private if you want. 
