Hi Guys,
I have been always pretty high on Haemoglobin and HCT since I'm young. it fluctuates from 16-17,5 and HCT from 46-49. I'm now older and at 17,9 HB and 52% HCT. I have seen 2 haematologists who are not worried about my result and said I'm not qualifying for PV and didn't want to test further. The issue is I have symptoms since a long time that I attribute to stress like being dizzy during the day while doing something and with being tired/weak all the time. I have seen that could be some symptoms of PV and I would like to know if there is something I could do expect Blood letting to lower my haemoglobin like supplements or anything's else. I start pomelo to lower HCT, recently.
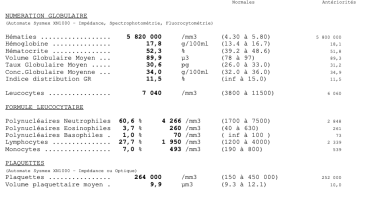
Here are my result, it's in French, but I assume you will understand. Thanks for your help, guys. Would be interested to have your opinions @Hans as I found all of your post really helpful.
I have been always pretty high on Haemoglobin and HCT since I'm young. it fluctuates from 16-17,5 and HCT from 46-49. I'm now older and at 17,9 HB and 52% HCT. I have seen 2 haematologists who are not worried about my result and said I'm not qualifying for PV and didn't want to test further. The issue is I have symptoms since a long time that I attribute to stress like being dizzy during the day while doing something and with being tired/weak all the time. I have seen that could be some symptoms of PV and I would like to know if there is something I could do expect Blood letting to lower my haemoglobin like supplements or anything's else. I start pomelo to lower HCT, recently.
Here are my result, it's in French, but I assume you will understand. Thanks for your help, guys. Would be interested to have your opinions @Hans as I found all of your post really helpful.