SOMO
Member
- Joined
- Mar 27, 2018
- Messages
- 1,094
Note: This topic is NOT about the CONSUMPTION/INTERNAL use of unsaturated fats. I do not believe anyone should consume vegetable oils due to their inherent stability , but this topic deals with the TOPICAL administration of these oils directly to the skin. I also don't believe applying topical oils will make anyone "fatter" by increasing the amount of total fat in the body.
___________________________________

I believe it has been shown with some certainty that topical (to the skin) application of FATTY ACIDS PENETRATE THE SKIN and can enter systemic circulation (or, at a bare minimum the epidermal top skin layer.) Different fatty acids penetrate the skin with different strength, with Oleic Acid being the best penetration enhancer and is commonly used in beauty products/cosmetics/skincare products/etc.
Ray Peat on his topical administration of lipid compounds (Vit D in this case) :
"Some people with very sensitive thin skin might absorb as much as 30 or 40 percent of what they put on...and yeah in the winter I try to do it every day."
There is research dating back decades that acne = LINOLEIC-ACID DEFICIENCY (Different than an Essential Fatty Acid Deficiency.) I repeat, an LA deficiency in the SKIN (if it exists) is different than a systemic EFA deficiency. The sebum of acne-sufferers. Nobody is more attractive because of acne and subconsciously when we see someone with acne, we are seeing how dysregulated that person's biology/health is. Acne is a serious health problem that manifests as an aesthetic issue and our society is concerned with appearance so it is reasonable to assume that if someone has acne they would want to get rid of it. Topical application of oils could potentially "Cure", not just "Reduce" acne.
I've read many anecdotes of people reducing skin issues (acne or hair/scalp problems) by TOPICAL application of these unstable unsaturated oils. Ray Peat talks about the body producing "Mead Acid" (an omega-9), so I speculate that people with messed up lipid peroxidation (if your skin is acne-prone it's almost certainly an issue of lipid peroxidation within your skin.)
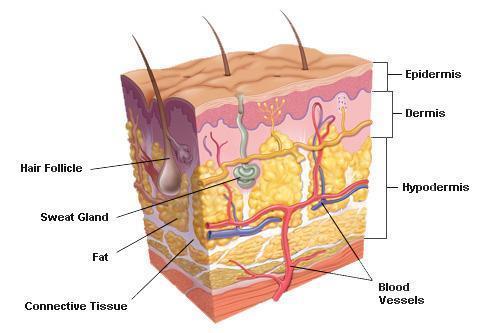
In this diagram of the skin-layers, there is a lot of "room" between the blood-vessels and the epidermis. There are numerous opportunities for the skin-cell shedding cycle to screw up along various phases of the shedding "cycle". Eating a clean diet itself can usually ward off acne in those that are acne-prone. Dairy is commonly linked with acne: (Acne and dairy products in adolescence: results from a Norwegian longitudinal study. - PubMed - NCBI)
Is it possible that Linoleic Acid, functioning as an IMMUNOSUPPRESSIVE, is "quieting" or silencing the inflammatory reaction in the skin?
Oleic Acid: (found in Olive Oil)
Ricinoleic Acid: (found in Castor Oil)
Linoleic Acid: (Any Vegetable oil basically, including soy and corn. )
Linoleic Acid/Pumpkin Seed Oil:
Used for Androgenic Alopecia, indicating it is blocking DHT. Regardless of the mechanism, it seems to be absorbed enough to affect the scalp cells.
Effect of Pumpkin Seed Oil on Hair Growth in Men with Androgenetic Alopecia: A Randomized, Double-Blind, Placebo-Controlled Trial
Linoleic Acid/Corn Oil:
Gamma-Linoleic Acid: (Hemp Oil/Evening Primrose Oil/Borage Oil)
-------------
Alternavista from acne.org (original topic: Acne Prone Skin/sebum Deficient In Linoleic Acid, Possible Topical Solution)
has compiled an impressive resource showing that Acne-prone skin (the sebum component of skin specifically) uses OLEIC ACID (an Omega-9, like Mead-Acid which Peat believes is naturally produced and resistant to lipid-peroxidation. Olive Oil is high in Omega-9 oleic acid.) instead of LINOLEIC ACID (Safflower/Soybean/Corn Oil) leading to hyperkeratinazation and "stickier" or more "rigid" sebum. This rigid sebum is then speculated to get "stuck" in the skin/hair follicle, leading to a buildup of cellular debris and eventually a localized minor irritation and/or infection, which rises to the epidermis and causes a visible whitehead. She has compiled the information in a more organized manner than this topic, and I recognize this topic will not change anyone's mind. But I do think it is possible that these oils may have benefits, as long as they are not consumed. I also noticed much of the research is focused on "receptors" and I don't think that's going to provide any solutions for people who actually suffer from acne right now.
-------
Oils and fatty acids are definitely absorbed through the skin to some degree and they seem to benefit vulnerable populations (with skin issues.)
Acne is an indicator that something in the person's diet or biology or both is irritating their skin. Topically applied oils do not seem to irritate skin, but orally ingested oils do for many people.
What are some DOWNSIDES of applying fats/oils/fatty-acids topically?
___________________________________
I believe it has been shown with some certainty that topical (to the skin) application of FATTY ACIDS PENETRATE THE SKIN and can enter systemic circulation (or, at a bare minimum the epidermal top skin layer.) Different fatty acids penetrate the skin with different strength, with Oleic Acid being the best penetration enhancer and is commonly used in beauty products/cosmetics/skincare products/etc.
Ray Peat on his topical administration of lipid compounds (Vit D in this case) :
"Some people with very sensitive thin skin might absorb as much as 30 or 40 percent of what they put on...and yeah in the winter I try to do it every day."
In AV, increased sebum flow dilutes linoleic acid resulting in a relative deficiency which may play a role in comedogenesis.
Acne Vulgaris and the Epidermal Barrier: Is Acne Vulgaris Associated with Inherent Epidermal Abnormalities that Cause Impairment of Barrier Functions? Do Any Topical Acne Therapies Alter the Structural and/or Functional Integrity of the Epidermal Barrier?
There is research dating back decades that acne = LINOLEIC-ACID DEFICIENCY (Different than an Essential Fatty Acid Deficiency.) I repeat, an LA deficiency in the SKIN (if it exists) is different than a systemic EFA deficiency. The sebum of acne-sufferers. Nobody is more attractive because of acne and subconsciously when we see someone with acne, we are seeing how dysregulated that person's biology/health is. Acne is a serious health problem that manifests as an aesthetic issue and our society is concerned with appearance so it is reasonable to assume that if someone has acne they would want to get rid of it. Topical application of oils could potentially "Cure", not just "Reduce" acne.
I've read many anecdotes of people reducing skin issues (acne or hair/scalp problems) by TOPICAL application of these unstable unsaturated oils. Ray Peat talks about the body producing "Mead Acid" (an omega-9), so I speculate that people with messed up lipid peroxidation (if your skin is acne-prone it's almost certainly an issue of lipid peroxidation within your skin.)
In this diagram of the skin-layers, there is a lot of "room" between the blood-vessels and the epidermis. There are numerous opportunities for the skin-cell shedding cycle to screw up along various phases of the shedding "cycle". Eating a clean diet itself can usually ward off acne in those that are acne-prone. Dairy is commonly linked with acne: (Acne and dairy products in adolescence: results from a Norwegian longitudinal study. - PubMed - NCBI)
Healing fats of the skin: the structural and immunologic roles of the omega-6 and omega-3 fatty acids.
Linoleic acid (18:2omega6) and alpha-linolenic
acid (18:3omega3) represent the parent fats of the two main classes of polyunsaturated fatty acids: the omega-6 (n-6) and the omega-3 (n-3) fatty acids, respectively. Linoleic acid and alpha-linolenic acid both give rise to other long-chain fatty acid derivatives, including gamma-linolenic acid and arachidonic acid (omega-6 fatty acids) and docosahexaenoic acid and eicosapentaenoic acid (omega-3 fatty acids). These fatty acids are showing promise as safe adjunctive treatments for many skin disorders, including atopic dermatitis, psoriasis, acne vulgaris, systemic lupus erythematosus, nonmelanoma skin cancer, and melanoma. Their roles are diverse and include maintenance of the stratum corneum permeability barrier, maturation and differentiation of the stratum corneum, formation and secretion of lamellar bodies, inhibition of proinflammatory eicosanoids, elevation of the sunburn threshold, inhibition of proinflammatory cytokines (tumor necrosis factor-alpha, interferon-gamma, and interleukin-12), inhibition of lipoxygenase, promotion of wound healing, and promotion of apoptosis in malignant cells, including melanoma. They fulfill these functions independently and through the modulation of peroxisome proliferator-activated and Toll-like receptors.
Healing fats of the skin: the structural and immunologic roles of the omega-6 and omega-3 fatty acids. - PubMed - NCBI
Is it possible that Linoleic Acid, functioning as an IMMUNOSUPPRESSIVE, is "quieting" or silencing the inflammatory reaction in the skin?
Oils/Fatty Acids and Effects of Topical Administration.
Oleic Acid: (found in Olive Oil)
With the exception of Limonene, I believe all the other chemicals are lipid-like or derived from lipids.The use of microemulsions is advantageous not only due to the facile and low cost preparation, but also because of the improved bioavailability. The increased absorption of drugs in topical applications is attributed to enhancement of penetration through the skin by the carrier. Saturated and unsaturated fatty acids serving as an oil phase are frequently used as penetration enhancers. The most popular enhancer is oleic acid. Other permeation enhancers commonly used in transdermal formulations are isopropyl myristate, isopropyl palmitate, triacetin, isostearylic isostearate, R(+)-limonene and medium chain triglycerides.
Microemulsions as transdermal drug delivery vehicles. - PubMed - NCBI
Oleic acid was found to be the most effective enhancer tested, increasing the percutaneous absorption of DHE by 208-fold.
Influence of oleic acid and other permeation promoters on transdermal delivery of dihydroergotamine through rabbit skin - ScienceDirect
---For example, oleic acid is a constituent of an estradiol transdermal formulation Vivelle® acting as a permeation enhancer in the presence of propylene glycol (propylene glycol itself is also a penetration enhancer and is slightly oily in texture so it is considered a "moisturizer".)
Efficiency of Fatty Acids as Chemical Penetration Enhancers: Mechanisms and Structure Enhancement Relationship
Ricinoleic Acid: (found in Castor Oil)
---Castor oil and Ricinoleic Acid can enhance the transdermal penetration of other chemicals.Final report on the safety assessment of Ricinus Communis (Castor) Seed Oil, Hydrogenated Castor Oil, Glyceryl Ricinoleate, Glyceryl Ricinoleate SE, ... - PubMed - NCBI
Mixture additives inhibit the dermal permeation of the fatty acid, ricinoleic acid. - PubMed - NCBI
Linoleic Acid: (Any Vegetable oil basically, including soy and corn. )
There was a significant effect of topically applied linoleic acid on the size of follicular casts and microcomedones, an almost 25% reduction in their overall size being achieved over a 1-month treatment period. In contrast, no change was found at placebo-treated sites
Digital image analysis of the effect of topically applied linoleic acid on acne microcomedones. - PubMed - NCBI
Linoleic Acid/Pumpkin Seed Oil:
Used for Androgenic Alopecia, indicating it is blocking DHT. Regardless of the mechanism, it seems to be absorbed enough to affect the scalp cells.
Effect of Pumpkin Seed Oil on Hair Growth in Men with Androgenetic Alopecia: A Randomized, Double-Blind, Placebo-Controlled Trial
Linoleic Acid/Corn Oil:
In vivo studies were conducted with curcumin (15 mg) suspended in vehicle (100 μL corn oil) for oral gavage feeding or suspended in a vanishing cream paste (15 mg/100 μL cream) for topical administration provided by our study compounding pharmacist (DB).
Topical corn oil in the management of essential fatty acid deficiency. - PubMed - NCBI
Gamma-Linoleic Acid: (Hemp Oil/Evening Primrose Oil/Borage Oil)
There is a greater antipruritic effect of GLA based on evaluation with both the VAS and PS. There is persistence of a residual effect into the second treatment period after GLA treatment.
-------------
Alternavista from acne.org (original topic: Acne Prone Skin/sebum Deficient In Linoleic Acid, Possible Topical Solution)
has compiled an impressive resource showing that Acne-prone skin (the sebum component of skin specifically) uses OLEIC ACID (an Omega-9, like Mead-Acid which Peat believes is naturally produced and resistant to lipid-peroxidation. Olive Oil is high in Omega-9 oleic acid.) instead of LINOLEIC ACID (Safflower/Soybean/Corn Oil) leading to hyperkeratinazation and "stickier" or more "rigid" sebum. This rigid sebum is then speculated to get "stuck" in the skin/hair follicle, leading to a buildup of cellular debris and eventually a localized minor irritation and/or infection, which rises to the epidermis and causes a visible whitehead. She has compiled the information in a more organized manner than this topic, and I recognize this topic will not change anyone's mind. But I do think it is possible that these oils may have benefits, as long as they are not consumed. I also noticed much of the research is focused on "receptors" and I don't think that's going to provide any solutions for people who actually suffer from acne right now.
-------
Oils and fatty acids are definitely absorbed through the skin to some degree and they seem to benefit vulnerable populations (with skin issues.)
Acne is an indicator that something in the person's diet or biology or both is irritating their skin. Topically applied oils do not seem to irritate skin, but orally ingested oils do for many people.
What are some DOWNSIDES of applying fats/oils/fatty-acids topically?




