bloom
Member
- Joined
- Feb 5, 2017
- Messages
- 184
Anyone whom has thoroughly looked into Post Finasteride Syndrome has come to the conclusion that 5ar is not functional in this condition. This is supported by empirical observations, and studies (while limited) on PFS.
The Latest study done on hormones in the CSF and plasma of PFS victims strongly suggest that 5ar is not functional. It found increased levels of Testosterone, with decreased levels of DHT, and DHP in the CSF. Along with an increase in Testosterone, a decrease in DHP, and Allopregnanolone, in the Plasma compared with controls.
Neuroactive steroid levels and psychiatric and andrological features in post-finasteride patients. - PubMed - NCBI
Many with PFS have reported (included myself) that they get better when they get sick. This study found that Cyclosporin A and immunosuppressant drug, increases peripheral 5ar activity. An interesting observation made by the authors was that there was not a significant change in plasma Androgen levels, I think this is a significant point and will come back to this.
Greater conversion of testosterone to 5 alpha-dihydrotestosterone, reflecting increased peripheral 5 alpha-reductase activity in nude mice treated ... - PubMed - NCBI
Guysswith PFS (including myself) report improvement of symptoms when taking a GABA A receptor agonist.
This study found that Valium (a GABA A receptor agonist), greatly increased the activity of 5ar in the Diencephalon of rats. Most metabolites of 5ar are potent GABA A receptor agonists:
Sex hormones metabolism in the brain: influence of central acting drugs on 5 alpha-reduction in rat diencephalon. - PubMed - NCBI
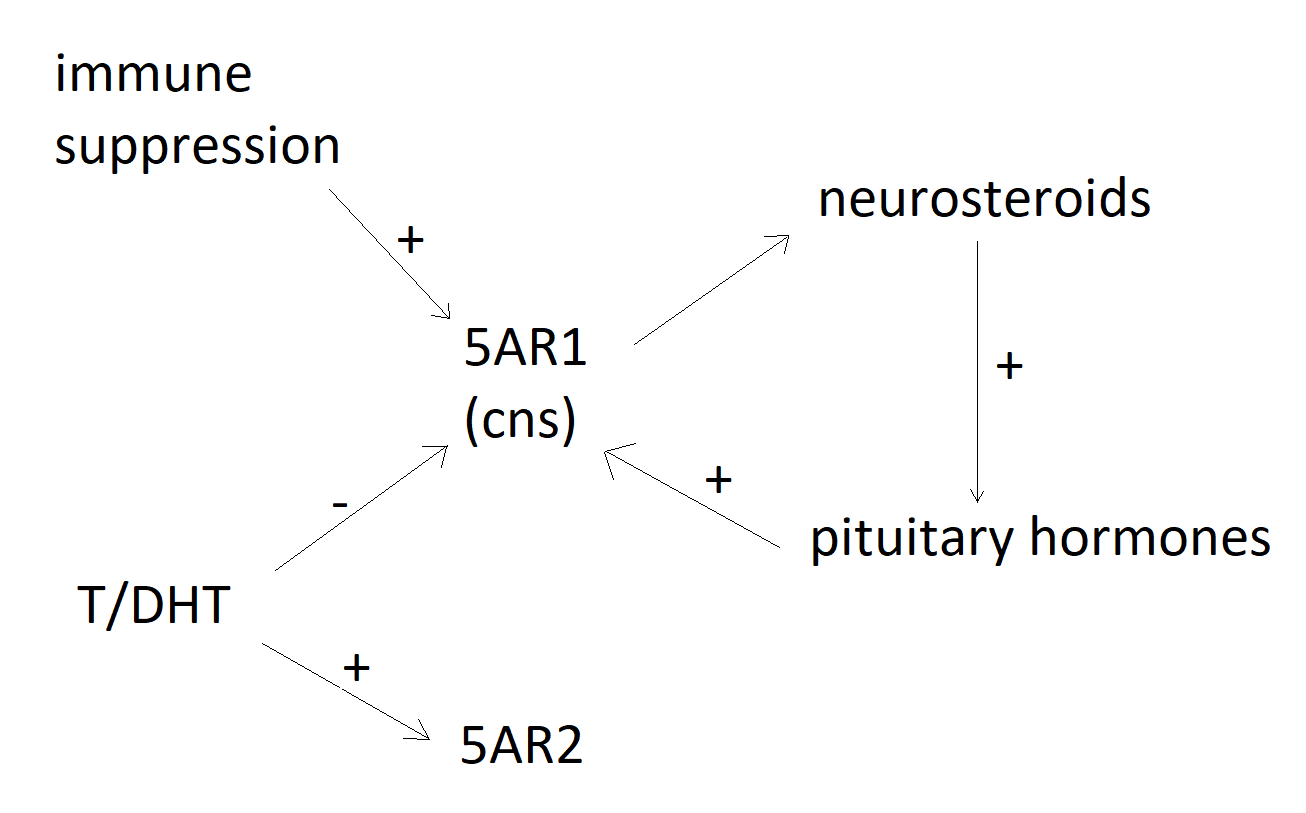
There are many known substances which can increase the activity of 5ar greatly. If it's the case that 5ar has been impaired or downregulated (as I believe it is in PFS), then why do a huge majority of guys report to get worse (including myself) when we increase Testosterone, DHT, and 5ar? The reason for this I believe is that while the 5ar2 isoenzyme appears to be under the positive gene expression of T/DHT. The gene expression of the 5ar1 isoenzyme appears to be under the NEGATIVE control of T/DHT, as this paper demonstrates.
file:///C:/Users/public.AUD54606QN-L76/Downloads/Differential_regulation_of_steroid_5alpha-reductas%20(1).pdf
It may very well be the case that in PFS 5ar1 has been downregulated, so any attempt to increase T/DHT may decrease the expression of an isoenzyme already downregulated. This can also explain why a significant number of guys get better when they have a suppressed immune system. The authors of the study which found that Cyclosporine A increased peripheral activity of 5ar in rats noted that Plasma levels of Androgens were not significantly changed. So it may be the case that there is no significant increase of these Androgens in the plasma to negatively regulate the 5ar1 isoenzyme in the CNS.
The theory that 5ar1 has been down regulated in PFS can also account for the strange reports of guys (including myself) claiming improvement when they go back on a 5ar inhibitor, and why guys (including myself) get worse when we increase T/DHT.
Interestingly while Androgens seems to positively regulate the expression of 5ar2, Pituitary hormones seem to positively regulate the gene expression of 5ar1.
Differential regulation of rat testicular 5alpha-reductase type 1 and 2 isoforms by testosterone and FSH. - PubMed - NCBI
Heterogeneity of rat type I 5 alpha-reductase cDNA: cloning, expression and regulation by pituitary implants and dihydrotestosterone. - PubMed - NCBI
This study found that Oxytocin a Pituitary Hormone Positively regulated the gene expression of 5ar1 but not 5ar2:
Oxytocin increases 5alpha-reductase activity of human prostate epithelial cells, but not stromal cells. - PubMed - NCBI
The question that arises now is, how has 5ar1 been down regulated in PFS? Especially considering that Finasteride does not significantly inhibit the 5ar1 isoenzyme.
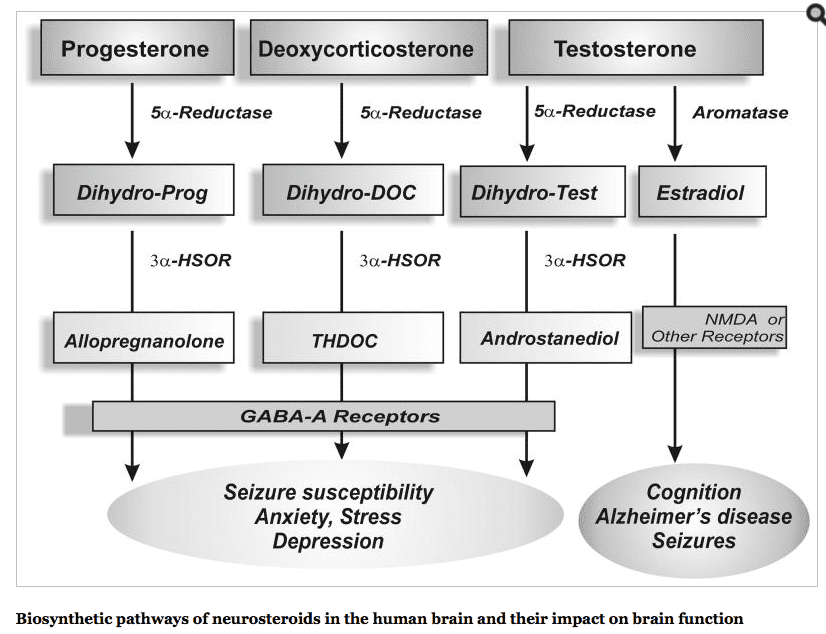
Inhibition of 5ar has been shown to dramatically reduce neurosteroids (especially Allopregnanolone).
This study found that Neurosteroids increased the release of Oxytocin in certain neurons, and that Allopregnanolone specifically increased the release of Vasopressin (another pituitary hormone).
Neurosteroid regulation of oxytocin and vasopressin release from the rat supraoptic nucleus. - PubMed - NCBI
It could be the case in PFS that reduction of neurosteroids (specifically Allopregnanolone) leads to a reduction of Oxytocin and Vasopressin, which leads to a reduction in 5ar1 expression. This reduction in 5ar1 expression consequently leads to a reduction of neurosteroid production, creating a vicious cycle. This could account for why we get better when we take things which are known to increase neurosteroids (i.e. Progesterone), and why we get better when we a lot of us take high doses of vitamin C, something known to significantly increase Oxytocin.
High-dose ascorbic acid increases intercourse frequency and improves mood: a randomized controlled clinical trial. - PubMed - NCBI
Oxytocin - Wikipedia
Considering that the latest study found that T/DHT levels were relatively normal in the PFS group. That guys generally get worse when increasing these Androgens. And that 5ar2 is under the positive gene expression of T/DHT. A more appropriate approach to PFS may be to increase 5ar1 activity, which may include focusing on Neurosteroids, and Pituitary Hormones since these seem to increase the gene expression of 5ar1. 5ar1 is an important part of the PFS puzzle I believe.
The Latest study done on hormones in the CSF and plasma of PFS victims strongly suggest that 5ar is not functional. It found increased levels of Testosterone, with decreased levels of DHT, and DHP in the CSF. Along with an increase in Testosterone, a decrease in DHP, and Allopregnanolone, in the Plasma compared with controls.
Neuroactive steroid levels and psychiatric and andrological features in post-finasteride patients. - PubMed - NCBI
levels of some neuroactive steroids analysed in CSF of PFS patients were significantly different versus those in healthy controls. In particular, the levels of PREG, as well as of its further metabolites, PROG and DHP, were significantly decreased in CSF of PFS patients. On the contrary, the levels of DHEA and T were significantly increased. The levels of metabolites of T, such as DHT, 3a-diol, and 17b-estradiol (17b-E) were also affected in CSF of PFS patients. In particular, we reported a decrease in the levels of DHT and 17b-E, associated with an increase in the 3a-diol levels.
In addition, the levels of PROG and T metabolites, such as DHT, 3a-diol, and 17b-E, were unaffected in plasma of PFS patients. Furthermore, the levels of THP that were unaffected in CSF, showed a significant decreased in plasma. In agreement to what observed in CSF, the plasma levels of DHEA and T showed a significant increase and those of DHP a significant decrease.
Many with PFS have reported (included myself) that they get better when they get sick. This study found that Cyclosporin A and immunosuppressant drug, increases peripheral 5ar activity. An interesting observation made by the authors was that there was not a significant change in plasma Androgen levels, I think this is a significant point and will come back to this.
Greater conversion of testosterone to 5 alpha-dihydrotestosterone, reflecting increased peripheral 5 alpha-reductase activity in nude mice treated ... - PubMed - NCBI
Following cyclosporine A (CsA) immunosuppressive therapy in kidney grafts, increased body hair growth (hypertrichosis and/or hirsutism) without significant variation in normal circulating plasma androgen levels (as observed in idiopathic hirsutism) has been reported by several authors. Other authors have described increased hair growth in nude mice treated with CsA.
After 1 h of incubation, 5 alpha-DHT and other 5 alpha-reduced products formed were separated and quantified using a reverse-phase chromatography column fitted to a flow-through radioactivity detector. Mean +/- SD 5 alpha-DHT formation (expressed as pmol per 100 mg of protein per h) was found to be increased in the treated groups (group 1: 3.17 +/- 0.37, group 2: 3.10 +/- 0.13, group 3: 4.26 +/- 0.20), respectively 7.5% (NS), 5.10% (NS) and 44.4% (P = 0.01) higher than in the control group (2.95 +/- 0.13). In addition to 5 alpha-DHT, enhanced formation of delta 4-androstenedione (delta 4), 5 alpha-androstan-3 beta,17 beta-diol (3 beta-diol) and 5 alpha-androstan-3 alpha,17 beta-diol (3 alpha-diol) were also observed in the treated groups. These results show a significantly increased formation of 5 alpha-DHT (and Adiol) in nude mice treated with high dose-levels of CsA.
Guysswith PFS (including myself) report improvement of symptoms when taking a GABA A receptor agonist.
This study found that Valium (a GABA A receptor agonist), greatly increased the activity of 5ar in the Diencephalon of rats. Most metabolites of 5ar are potent GABA A receptor agonists:
Sex hormones metabolism in the brain: influence of central acting drugs on 5 alpha-reduction in rat diencephalon. - PubMed - NCBI
"...Diencephalon 5 alpha-reductase activity showed a highly significant increase (p less than 0.01) after a single administration of carbamazepine, reserpine, diazepam, phenytoin, phenobarbital or disulfiram. A significant increase (p less than 0.05) was also found after a single administration of methylphenidate, caffeine or methamphetamine."
There are many known substances which can increase the activity of 5ar greatly. If it's the case that 5ar has been impaired or downregulated (as I believe it is in PFS), then why do a huge majority of guys report to get worse (including myself) when we increase Testosterone, DHT, and 5ar? The reason for this I believe is that while the 5ar2 isoenzyme appears to be under the positive gene expression of T/DHT. The gene expression of the 5ar1 isoenzyme appears to be under the NEGATIVE control of T/DHT, as this paper demonstrates.
file:///C:/Users/public.AUD54606QN-L76/Downloads/Differential_regulation_of_steroid_5alpha-reductas%20(1).pdf
The results of our experiment clearly demonstrate that both isozymes of 5-R are expressed in prefrontal cortex of adult male rats. It was previously reported that 5-R type 2 is selectively expressed in the hypothalamus
The pattern of expression of 5-R type 2 presented in this study appears to be correlated with T levels, indicating that this isozyme may be positively modulated by androgen, as described previously during late fetal/ early post-natal life (1). Our results demonstrate for the first time that 5-R type 2 expression in the brain is regulated by DHT, a product of the encoded enzyme, via a form of feed-forward regulation. This regulatory mechanism is common among developmentally important genes (19, 23). Thus, T and DHT bind to a transcription factor, the androgen receptor, which in turn activates genes that carry out morphogenetic programs implicated in sexual differentiation processes in specific brain regions (1).
Our study demonstrated that 5-R type 1 expression is not controlled by androgen in the intact animal. However, it is negatively controlled by some testicular factors (in part by T and DHT) because there is a marked increase in 5-R type 1 expression in castrated animals, in which circulating T and DHT are low. Furthermore, T and DHT decrease the mRNA levels of 5-R type 1 in castrated animals. These findings are novel and surprising
Our data demonstrated an increase in 5-R type 1 expression in the castrated male rat that is hormonally similar to a female model. This observation is consistent with a previous report that 5-R activity in liver, which expresses only 5-R type 1, is more active in female than in male rats (34).
To our best knowledge, our study provides the first evidence that the expression of both 5-R isozymes in the brain, at least in the cerebral cortex, is regulated in opposite ways by androgens. This finding suggests that both isozymes may play a role in the sexual dimorphism of the CNS, besides other functions.
It may very well be the case that in PFS 5ar1 has been downregulated, so any attempt to increase T/DHT may decrease the expression of an isoenzyme already downregulated. This can also explain why a significant number of guys get better when they have a suppressed immune system. The authors of the study which found that Cyclosporine A increased peripheral activity of 5ar in rats noted that Plasma levels of Androgens were not significantly changed. So it may be the case that there is no significant increase of these Androgens in the plasma to negatively regulate the 5ar1 isoenzyme in the CNS.
The theory that 5ar1 has been down regulated in PFS can also account for the strange reports of guys (including myself) claiming improvement when they go back on a 5ar inhibitor, and why guys (including myself) get worse when we increase T/DHT.
Interestingly while Androgens seems to positively regulate the expression of 5ar2, Pituitary hormones seem to positively regulate the gene expression of 5ar1.
Differential regulation of rat testicular 5alpha-reductase type 1 and 2 isoforms by testosterone and FSH. - PubMed - NCBI
5alphaR-1 mRNA and enzyme activity increased when testosterone was suppressed, yet restoration of testosterone decreased 5alphaR-1 mRNA and enzyme activity, suggesting that testosterone negatively regulates 5alphaR-1. suppression of FSH decreased 5alphaR-1 mRNA yet FSH administration increased 5alphaR-1 mRNA, but no changes in 5alphaR-1 activity were observed within the 6 day period.
It is concluded that the 5alphaR isoforms in rat testis are differentially regulated by testosterone and FSH: testosterone negatively regulated 5alphaR-1 mRNA and enzyme activity but had no affect on 5alphaR-2, whereas FSH positively regulated 5alphaR-1 mRNA and appeared to regulate 5alphaR-2.
Heterogeneity of rat type I 5 alpha-reductase cDNA: cloning, expression and regulation by pituitary implants and dihydrotestosterone. - PubMed - NCBI
To determine the effect of pituitary hormones and dihydrotestosterone (DHT), the mRNA levels in the livers of rats treated with pituitary implants, hypophysectomized, castrated, and castrated coupled with DHT treatment were quantified by dot-blot hybridization assay using rat type I 5 alpha-reductase cDNA as probes. The results demonstrated that rat type I 5 alpha-reductase mRNA is stimulated by pituitary hormones and castration but is decreased by DHT and hypophysectomy.
This study found that Oxytocin a Pituitary Hormone Positively regulated the gene expression of 5ar1 but not 5ar2:
Oxytocin increases 5alpha-reductase activity of human prostate epithelial cells, but not stromal cells. - PubMed - NCBI
Oxytocin significantly increased the total 5-alpha-reductase activity of PrEC but not of PrSC. 5-alpha-Reductase I gene expression and enzyme activity were also increased (P<0.05) in PrEC by oxytocin. Oxytocin significantly increased type II activity, but not expression, in PrEC. Oxytocin did not significantly affect 5-alpha-reductase activity or expression in PrSC.
The question that arises now is, how has 5ar1 been down regulated in PFS? Especially considering that Finasteride does not significantly inhibit the 5ar1 isoenzyme.
Inhibition of 5ar has been shown to dramatically reduce neurosteroids (especially Allopregnanolone).
This study found that Neurosteroids increased the release of Oxytocin in certain neurons, and that Allopregnanolone specifically increased the release of Vasopressin (another pituitary hormone).
Neurosteroid regulation of oxytocin and vasopressin release from the rat supraoptic nucleus. - PubMed - NCBI
In the adult, oxytocin effects are modulated by allopregnanolone via an interaction with inhibitory GABAA receptors. This study examined the effects of allopregnanolone, progesterone and 17beta-oestradiol on oxytocin and vasopressin release from intact isolated supraoptic nuclei and from the neurophypophyses in rats of differing ages. In supraoptic nuclei from rats of 3-4 weeks old or less, all three neurosteroids induced oxytocin release from the isolated supraoptic nucleus, but only allopregnanolone induced significant release of vasopressin. Surprisingly, in these very young rats, allopregnanolone-induced oxytocin release was inhibited by GABAA receptor antagonists as well as by an oxytocin receptor antagonist
It could be the case in PFS that reduction of neurosteroids (specifically Allopregnanolone) leads to a reduction of Oxytocin and Vasopressin, which leads to a reduction in 5ar1 expression. This reduction in 5ar1 expression consequently leads to a reduction of neurosteroid production, creating a vicious cycle. This could account for why we get better when we take things which are known to increase neurosteroids (i.e. Progesterone), and why we get better when we a lot of us take high doses of vitamin C, something known to significantly increase Oxytocin.
High-dose ascorbic acid increases intercourse frequency and improves mood: a randomized controlled clinical trial. - PubMed - NCBI
Ascorbic acid (AA) modulates catecholaminergic activity, decreases stress reactivity, approach anxiety and prolactin release, improves vascular function, and increases oxytocin release. These processes are relevant to sexual behavior and mood
The AA group reported greater FSI (but, as hypothesized, not other sexual behavior) frequency, an effect most prominent in subjects not cohabiting with their sexual partner, and in women. The AA but not placebo group also experienced a decrease in Beck Depression scores.
Oxytocin - Wikipedia
The activity of the PAM enzyme system is dependent upon vitamin C (ascorbate), which is a necessary vitamin cofactor. By chance, sodium ascorbate by itself was found to stimulate the production of oxytocin from ovarian tissue over a range of concentrations in a dose-dependent manner.[21] Many of the same tissues (e.g. ovaries, testes, eyes, adrenals, placenta, thymus, pancreas) where PAM (and oxytocin by default) is found are also known to store higher concentrations of vitamin C.[22]
Considering that the latest study found that T/DHT levels were relatively normal in the PFS group. That guys generally get worse when increasing these Androgens. And that 5ar2 is under the positive gene expression of T/DHT. A more appropriate approach to PFS may be to increase 5ar1 activity, which may include focusing on Neurosteroids, and Pituitary Hormones since these seem to increase the gene expression of 5ar1. 5ar1 is an important part of the PFS puzzle I believe.
Last edited: