I also learned quite a bit about magnesium over the years.
I'm still convinced that magnesium is the most important supplement for my son. After trying a lot of different forms and dosages of magnesium we are currently giving him 275mg elemental magnesium in two divided doses from the following magnesium forms:
45mg from magnesium N-acetyltaurinate (pure powder from mind nutrition)
100mg from magnesium taurinate (pure powder from yango)
130mg from magnesium bisglycinate (pure powder Albion taste free version sold by nutrixeal)
I think that magnesium N-acetyltaurinate is probably the most potent form of magnesium for seizures. Mind nutrition writes on their website, "the acetylation of taurine removes the zwitterion structure of taurine, providing ATA Mg® with a lipophilic character which facilitates membrane phospholipids passage and cell penetration for both magnesium and taurine, in particular into neuronal cells."
This is supported by a rat study showing that, compared to magnesium sulfate, oxide, malate, and citrate, magnesium N-acetyltaurinate led to the highest accumulation of magnesium in the brain:
In a second study, the investigators compared the bioavailability of different doses of magnesium malate, citrate, acetytaurinate, and glycinate. Again, the acetyltaurinate form increased brain magnesium the most and it was effective even at the low dose.
Accordingly, magnesium acetyl-taurinate was found to be the most effective form of magnesium for seizures in another aninmal study. In this study, the investigators studied the effects of magnesium acetlytaurinate, magnesium pyrrolidone-2-carboxylate (which is the same as magnesium pidolate contained in Haiduts magnoil), and magnesium chloride alone and in combination with vitamin B6 on audiogenic seizures in magnesium deficient mice. Magnesium acetyltaurinate was the most fast acting form of magnesium and unlike other forms of magnesium its effects were permanent. B6 helped to increase the efficacy of other forms:
And here is another animal study supporting the efficacy of magnesium acetyl-taurinate
The reason why magnesium acetyltaurinate might be the best form of magnesium for seizures is that it not only provides magnesium to the brain but also taurine, which is anticonvulsive in itself (at least in animals). Here are some interesting review papers:

 pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
 www.sciencedirect.com
www.sciencedirect.com

 www.ncbi.nlm.nih.gov
www.ncbi.nlm.nih.gov
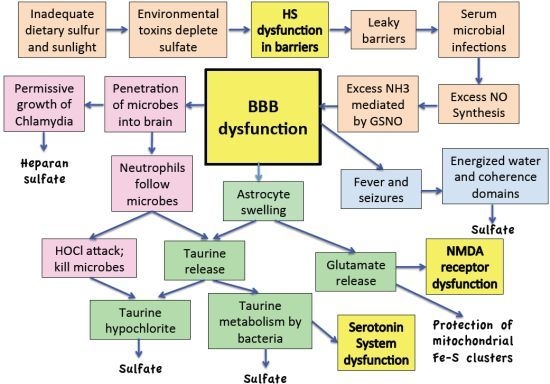
An interesting theory is also provided by Stefanie Seneff. She postulated in this paper that seizures serve the function to renew sulfate supply in the brain and that taurine may provide an alternative source for sulfate renewal:
 www.mdpi.com
www.mdpi.com
Interestingly, taurine is also helpful to get rid of ammonia and it seems to synergize well with alpha-ketoglutaric acid. Jon Pangborn writes: "Alpha-ketoglutaric acid does not stop excessive formation of ammonia, rather, it extends cell and tissue abilities to cope with ammonia. It chemically combines with ammonia to form glutamic acid - a much less toxic substance than ammonia. If ammonia excess is the problem, gram quantities per day of alpha-ketoglutarate (buffered) can be beneficial 50 to 200 mg per Kg body weight. A taurine supplement might help further by encouraging the conversion of glutamic acid to glutamine."
However, I have to say that I also read all human studies that have tested the effect of taurine on seizures and, unfortunately, the results are mixed. Most of these studies were conducted in the seventies and early eighties in Italy and probably due to the mixed results have not been followed up.
 www.karger.com
pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
www.karger.com
pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
A common finding of these studies was that taurine was quite effective at the beginning but that this effect was lost over time.
Nevertheless, my personal experience with magnesium N-acetyltaurinate and magnesium taurinate is that it is very helpful even in the longer term. For a while, we had replaced magnesium taurinate with other forms of magnesium and only kept the relatively small dose magnesium-N-acetyltaurinate. My son seems to be doing much better if he gets more taurine from magnesium taurinate.
The reason why I do not give everything as magnesium N-acetyltaurinate but also add regular magnesium taurinate to the mix is that magnesium N-acetyltaurinate has a very bitter taste and my son cannot swallow capsules. Conversely, regular magnesium taurinate has a neutral taste, it's well soluble in water and it's also much cheaper.
The other magnesium form I'm still a big fan of is magnesium glycinate. Earlier in the thread, I was concerned that glycine might be problematic because my son might have nonketotic hyperglycinemia. However, we have later ruled out this possibility. I think magnesium glycinate is one of the best forms for my son because it's extremely well absorbed and because glycine has various other health benefits, including protecting the liver and increasing glutathione production.
One problem that I had with magnesium glycinate though was it's very bad fishy after taste and so it was a struggle to give it to my son. Only about 1 year ago I discovered thanks to a Ray Peat forum member, that a French supplement shop called Nutrixeal sells the pure poweder of Albion's taste free version of magnesium bisglycinate. Apparently, this version of magnesium glycinate is more purified and it also seems to be more fully reacted. That is, it seems to contain less unreacted magnesium oxide. That's why this version of magnesium glycinate contains only 8% elemental magnesium whereas the regular magnesium bisglycinate from Albion contains 10% elemental magnesium. I can attest that the taste free version of magnesium glycinate has almost no taste and that there is a huge difference to the regular form. It's a shame that the taste free version is not more widely available. The only other company that I know that sells the taste free version is Thorne, but they do not sell the pure powder and add monk fruit extract and citric acid to it.
For a while, we also supplemented magnesium in the form of magnesium creatinate because, as I had already mentioned in my email to Ray Peat, there is some animal research indicating that valproic acid is interfering with creatine production and creatine has been shown to be anticonvulsive in various animal models of epilepsy. Magnesium creatine has also the advantage that it is well soluble in water and has almost no taste. However, although there were no negative effects as far as I can tell, it's my impression that magnesium taurinate is more benefical and so we replaced it with the latter.
We also tried magnesium threonate and magnesium malate. I think these are good forms as well, but I think magnesium N-acetyltaurinate, magnesium taurinate and magnesium bisglycinate are superior.
Magnesium pidolate might be another very good form for seizures, although we have not tried it. One study found that it "was the most efficient in reducing the permeability [of the blood brain barrier] and in enhancing magnesium transport through the barrier." This is important because the blood brain barrier is well known to be impaired in epilepsy:
pubmed.ncbi.nlm.nih.gov
Apart from that, magnesium pidolate has been demonstrated to be one of the most effective magnesium forms for preventing seizures in animals (see studies above) and it has been widely and successully used (particularly in Italy and France) for the prevention of migraine and tension headaches in children, which I take as a very good sign because migraine and epilepsy have many things in common and what works for migraines usually also works for seizures.
pubmed.ncbi.nlm.nih.gov
I'm still convinced that magnesium is the most important supplement for my son. After trying a lot of different forms and dosages of magnesium we are currently giving him 275mg elemental magnesium in two divided doses from the following magnesium forms:
45mg from magnesium N-acetyltaurinate (pure powder from mind nutrition)
100mg from magnesium taurinate (pure powder from yango)
130mg from magnesium bisglycinate (pure powder Albion taste free version sold by nutrixeal)
I think that magnesium N-acetyltaurinate is probably the most potent form of magnesium for seizures. Mind nutrition writes on their website, "the acetylation of taurine removes the zwitterion structure of taurine, providing ATA Mg® with a lipophilic character which facilitates membrane phospholipids passage and cell penetration for both magnesium and taurine, in particular into neuronal cells."
This is supported by a rat study showing that, compared to magnesium sulfate, oxide, malate, and citrate, magnesium N-acetyltaurinate led to the highest accumulation of magnesium in the brain:
Timeline (Bioavailability) of Magnesium Compounds in Hours: Which Magnesium Compound Works Best?
Nazan Uysal 1 2, Servet Kizildag 3, Zeynep Yuce 4, Guven Guvendi 5, Sevim Kandis 5, Basar Koc 5, Aslı Karakilic 5, Ulas M Camsari 6, Mehmet Ates 3
Abstract
Magnesium is an element of great importance functioning because of its association with many cellular physiological functions. The magnesium content of foods is gradually decreasing due to food processing, and magnesium supplementation for healthy living has become increasingly popular. However, data is very limited on the bioavailability of various magnesium preparations. The aim of this study is to investigate the bioavailability of five different magnesium compounds (magnesium sulfate, magnesium oxide, magnesium acetyl taurate, magnesium citrate, and magnesium malate) in different tissues. Following a single dose 400 mg/70 kg magnesium administration to Sprague Dawley rats, bioavailability was evaluated by examining time-dependent absorption, tissue penetration, and the effects on the behavior of the animals. Pharmacokinetically, the area under the curve calculation is highest in the magnesium malate. The magnesium acetyl taurate was found to have the second highest area under the curve calculation. Magnesium acetyl taurate was rapidly absorbed, able to pass through to the brain easily, had the highest tissue concentration level in the brain, and was found to be associated with decreased anxiety indicators. Magnesium malate levels remained high for an extended period of time in the serum. The commonly prescribed dietary supplements magnesium oxide and magnesium citrate had the lowest bioavailability when compared to our control group. More research is needed to investigate the bioavailability of magnesium malate and acetyl taurate compounds and their effects in specific tissues and on behavior.
In a second study, the investigators compared the bioavailability of different doses of magnesium malate, citrate, acetytaurinate, and glycinate. Again, the acetyltaurinate form increased brain magnesium the most and it was effective even at the low dose.
Biol Trace Elem Res
2019 Dec;192(2):244-251.
doi: 10.1007/s12011-019-01663-0. Epub 2019 Feb 13.
Dose-Dependent Absorption Profile of Different Magnesium Compounds
Mehmet Ates 1, Servet Kizildag 1, Oguz Yuksel 2, Ferda Hosgorler 3, Zeynep Yuce 4, Guven Guvendi 3, Sevim Kandis 3, Aslı Karakilic 3, Basar Koc 3, Nazan Uysal 5
Abstract
Magnesium, one of the basic elements for the human body, is necessary for many physiological functions. Magnesium deficiency is widely observed as a result of the reduced nutrient content of foods, over-cooking, diseases, drugs, alcohol, and caffeine consumption. Taking a dietary supplement is necessary magnesium deficiency. It has been demonstrated that absorption of organic magnesium compounds is better than absorption of inorganic compounds. The aim of this study is to investigate transitions to tissues of different organic magnesium compounds in different doses and whether there is a difference in the organic acid-bounded compounds (magnesium citrate and magnesium malate) and the amino acid-bounded compounds (magnesium acetyl taurate and magnesium glycinate), associated with transition and bioavailability. In addition, the effects of split dosages of high doses in a high volume of solvent on tissue magnesium levels are being investigated, because galenic formulation problems are regarded to prepare convenient dosage that can be taken once a day. All magnesium compounds were administered as three different doses, 45, 135, and 405 mg/70 kg elemental magnesium, were given per orally to Balbc mice. In a second set of experiments, 405 mg/70 kg high dose was divided into two doses of 202.5 mg/70 kg each and administered every 12 h. Brain, muscle tissues, and serum magnesium levels measured in all experimental groups and control 24 h later. Brain magnesium levels were found increased in all magnesium acetyl taurate administered subjects. Magnesium citrate increased muscle and brain magnesium levels in a dose-independent manner. We showed that dividing high doses of daily administered magnesium compounds did not sufficiently increase tissue magnesium levels. Although passive paracellular mechanism by solvent drag is the main mechanism of Mg absorption, other factors (electrochemical gradient effects, transcellular transporter mechanisms, magnesium status) should be effective on our results. It is necessary for further research on long-term administration of different magnesium compounds and their effect on other tissues.
Accordingly, magnesium acetyl-taurinate was found to be the most effective form of magnesium for seizures in another aninmal study. In this study, the investigators studied the effects of magnesium acetlytaurinate, magnesium pyrrolidone-2-carboxylate (which is the same as magnesium pidolate contained in Haiduts magnoil), and magnesium chloride alone and in combination with vitamin B6 on audiogenic seizures in magnesium deficient mice. Magnesium acetyltaurinate was the most fast acting form of magnesium and unlike other forms of magnesium its effects were permanent. B6 helped to increase the efficacy of other forms:
Audiogenic seizures in magnesium-deficient mice: effects of magnesium pyrrolidone-2-carboxylate, magnesium acetyltaurinate, magnesium chloride and vitamin B-6
Pierre Bac1, Christine Herrenknecht, Pierre Binet1 and Jean Durlach2
1Faculté de Pharmacie, rue J.B. C1ément; 2S.D.R.M. Hôpital Saint-Vincent de Paul, Avenue Denfert-Rochereau, Paris, France
Summary: Magnesium deficiency in mice causes and increases audiogenic seizures. This effect was reversed by oral administration of magnesium acetyltaurinate (ATaMg), magnesium pyrrolidone-2-carboxylate (PCMH), MgCl2. When treatment was discontinued, audiogenic seizures recurred only in the groups treated with PCMH or MgCl2. Following intraperitoneal administration of AtaMg. the mice were protected against audiogenic seizures after 4 h and this protection persisted for up to 72 h after the treatment. With the other magnesium salts (PCMH and MgCl2) maximum protection occurred by 6 h after the injection, but after that time the number of seizures increased sharply. Intraperitoneal taurine alone only reduced the severity of the audiogenic seizures. The length of treatment needed to inhibit audiogenic seizures was reduced by treatment with a combination of vitamin B-6 (a magnesium fixing agent) and PCMH or MgCl2. However this combination of vitamin B-6 and magnesium salts did not prevent the recurrence of audiogenic seizures, which was only achieved by ATaMg.
The results suggest that audiogenic seizures in magnesium-deficient mice form a model of magnesium depletion. This depletion is completely inhibited by the combination of an inhibitory neurotransmitter (taurine) and magnesium, in the form of magnesium acetyltaurinate.
And here is another animal study supporting the efficacy of magnesium acetyl-taurinate
Reversible model of magnesium depletion induced by systemic kainic acid injection in magnesium-deficient rats: I--Comparative study of various magnesium salts
P Bac 1, C Herrenknecht, N Pagès, C Dupont, J Durlach
Abstract
We developed three models of reversible magnesium depletion in rats resulting from the combined effects of kainic (KA) acid with magnesium deficiency, in order to compare the effects of various common magnesium salts (pidolate, aspartate, lactate, gluconate and chloride) and of magnesium acetyl taurinate (MgATa), administered daily (14 mg Mg2+, PO) for ten days. First, the immediate effects (wet dog shakes, clonic convulsions and death 1 h after injection) and late effects (fall from hole board between the second and tenth days post injection) of kainic acid at three different doses (3.6 and 11 mg/kg) were studied in magnesium deficient rats (50 ppm for 40 days) and in non-deficient rats (1700 ppm). The results showed that the effects of kainic acid were enhanced in magnesium deficient rats. Secondly, after ten days of physiological then pharmacological doses of magnesium, used as chronical supplementation, we showed that kainic acid administration combined with magnesium deficiency led to magnesium depletion of increasing severity depending on the dose of kainic acid. The observed magnesium depletions were weak at a dose of 3 mg/kg KA, moderate at a dose of 6 mg/kg and severe at a dose of 11 mg/kg. These depletions were more or less reversible, and this enabled the classification of the therapeutic effects of these salts on Mg depletion. Among common salts, magnesium pidolate presented the greatest efficacy but none of them fully prevented depletion. In contrast, MgATa was efficient on all the aspects of depletion, when administered preventively both chronically or acutely or as a single curative injection. Consequently the results we obtained in the present study, on a new model of magnesium depletion, showed the greatest efficacy of magnesium acetyl taurinate we demonstrated yet on other models of reversible magnesium depletion.
The reason why magnesium acetyltaurinate might be the best form of magnesium for seizures is that it not only provides magnesium to the brain but also taurine, which is anticonvulsive in itself (at least in animals). Here are some interesting review papers:
Sulfur - Containing Amino Acids in Seizures: Current State of the Art - PubMed
In this article we addressed the role of homocysteine and its related metabolite homocysteine thiolactone in the development of seizures, focusing on its experimental models in vivo, potential mechanisms of proepileptogenic activity via interactions with glutamatergic neurotransmission, sodium...
pubmed.ncbi.nlm.nih.gov
Taurine and epilepsy - PubMed
Dysfunction of excitatory and inhibitory neurotransmitters or neuromodulators is thought to underlie epileptic symptoms. Taurine, 2-aminoethanesulfonate, is a ubiquitous free amino acid abounding in the brain of humans and most animal species. It hyperpolarizes neurons and inhibits their firing...
pubmed.ncbi.nlm.nih.gov
The Effects of Taurine Exposure on the Brain and Neurological Disorders
Taurine is present in the brain, where it appears to be involved in many functions from conception onward. It plays a role in neurotransmission, altho…
Effects and Mechanisms of Taurine as a Therapeutic Agent
Taurine is an abundant, β-amino acid with diverse cytoprotective activity. In some species, taurine is an essential nutrient but in man it is considered a semi-essential nutrient, although cells lacking taurine show major pathology. These findings ...
www.ncbi.nlm.nih.gov
An interesting theory is also provided by Stefanie Seneff. She postulated in this paper that seizures serve the function to renew sulfate supply in the brain and that taurine may provide an alternative source for sulfate renewal:
Is Encephalopathy a Mechanism to Renew Sulfate in Autism?
This paper makes two claims: (1) autism can be characterized as a chronic low-grade encephalopathy, associated with excess exposure to nitric oxide, ammonia and glutamate in the central nervous system, which leads to hippocampal pathologies and resulting cognitive impairment, and (2)...
Interestingly, taurine is also helpful to get rid of ammonia and it seems to synergize well with alpha-ketoglutaric acid. Jon Pangborn writes: "Alpha-ketoglutaric acid does not stop excessive formation of ammonia, rather, it extends cell and tissue abilities to cope with ammonia. It chemically combines with ammonia to form glutamic acid - a much less toxic substance than ammonia. If ammonia excess is the problem, gram quantities per day of alpha-ketoglutarate (buffered) can be beneficial 50 to 200 mg per Kg body weight. A taurine supplement might help further by encouraging the conversion of glutamic acid to glutamine."
However, I have to say that I also read all human studies that have tested the effect of taurine on seizures and, unfortunately, the results are mixed. Most of these studies were conducted in the seventies and early eighties in Italy and probably due to the mixed results have not been followed up.
First Clinical Experience on the Antiepileptic Action of Taurine
Abstract. On the basis of previous investigations showing the antiepileptic action of taurine in both acute and chronic experimental epileptogenic foci, taurine was administered intraperitoneally to 15 highly refractory patients presenting daily frequent seizures of various types. Taurine was...
www.karger.com
Therapeutic trial by taurine for intractable childhood epilepsies - PubMed
Taurine was administered orally to 25 intractable epileptic children, ranging in age from 4 months to 12 years. All patients had been suffered from frequent seizures daily in spite of vigorous anticonvulsant medication. Daily taurine doses ranged from 0.05 to 0.3 g/kg. Twelve patients received...
pubmed.ncbi.nlm.nih.gov
[Orally-administered taurine in therapy-resistant epilepsy (author's transl)] - PubMed
The anticonvulsive action of taurine, was tested in 9 therapy in 9 therapy-resistant patients with a high incidence of seizures. Taurine was given orally (1.5-7.5 g daily) over a period of 4 to 16 weeks and, despite the high dosage, no appreciable side effects were observed. During this time...
pubmed.ncbi.nlm.nih.gov
Effects of taurine on seizures and growth hormone release in epileptic patients - PubMed
Oral taurine at doses of 375 to 8,000 mg/day (16 to 150 mg/kg/day) was administered to six patients with mixed seizure disorders refractory to standard anticonvulsant treatment. No improvement in seizure control was observed. During taurine tolerance testing, a substantial rise in plasma growth...
pubmed.ncbi.nlm.nih.gov
[Therapeutic effects of taurine in epilepsy: a clinical and polyphysiographic study (author's transl)] - PubMed
A study was carried out after i.v. administration of 200 mg/Kg of taurine on 37 epileptic patients in whom frequency and duration of seizures was considerable. Twenty-two subjects were given taurine for 15 consecutive days and then, once a week for a period of 6 weeks. In 5 control cases, the...
pubmed.ncbi.nlm.nih.gov
[Clinical study on the control of epilepsy using taurine] - PubMed
The A., after a detailed examination of the researches carried out with taurine in the clinical pictures of epilepsy, has examined the encephalographic and subjective aspects in 19 epileptics, all patients at the Mental Hospital in Agrigento. In all of them he has noticed a clear aggravation of...
pubmed.ncbi.nlm.nih.gov
Biochemical observations following administration of taurine to patients with epilepsy - PubMed
Amino acid analysis of plasma and urine obtained from 12 patients with epilepsy indicated that the plasma concentrations of taurine and glutamic acid were much higher than might have been expected. Glutamic acid in urine was also increased in these patients. Oral administration of taurine did...
pubmed.ncbi.nlm.nih.gov
A common finding of these studies was that taurine was quite effective at the beginning but that this effect was lost over time.
Nevertheless, my personal experience with magnesium N-acetyltaurinate and magnesium taurinate is that it is very helpful even in the longer term. For a while, we had replaced magnesium taurinate with other forms of magnesium and only kept the relatively small dose magnesium-N-acetyltaurinate. My son seems to be doing much better if he gets more taurine from magnesium taurinate.
The reason why I do not give everything as magnesium N-acetyltaurinate but also add regular magnesium taurinate to the mix is that magnesium N-acetyltaurinate has a very bitter taste and my son cannot swallow capsules. Conversely, regular magnesium taurinate has a neutral taste, it's well soluble in water and it's also much cheaper.
The other magnesium form I'm still a big fan of is magnesium glycinate. Earlier in the thread, I was concerned that glycine might be problematic because my son might have nonketotic hyperglycinemia. However, we have later ruled out this possibility. I think magnesium glycinate is one of the best forms for my son because it's extremely well absorbed and because glycine has various other health benefits, including protecting the liver and increasing glutathione production.
One problem that I had with magnesium glycinate though was it's very bad fishy after taste and so it was a struggle to give it to my son. Only about 1 year ago I discovered thanks to a Ray Peat forum member, that a French supplement shop called Nutrixeal sells the pure poweder of Albion's taste free version of magnesium bisglycinate. Apparently, this version of magnesium glycinate is more purified and it also seems to be more fully reacted. That is, it seems to contain less unreacted magnesium oxide. That's why this version of magnesium glycinate contains only 8% elemental magnesium whereas the regular magnesium bisglycinate from Albion contains 10% elemental magnesium. I can attest that the taste free version of magnesium glycinate has almost no taste and that there is a huge difference to the regular form. It's a shame that the taste free version is not more widely available. The only other company that I know that sells the taste free version is Thorne, but they do not sell the pure powder and add monk fruit extract and citric acid to it.
For a while, we also supplemented magnesium in the form of magnesium creatinate because, as I had already mentioned in my email to Ray Peat, there is some animal research indicating that valproic acid is interfering with creatine production and creatine has been shown to be anticonvulsive in various animal models of epilepsy. Magnesium creatine has also the advantage that it is well soluble in water and has almost no taste. However, although there were no negative effects as far as I can tell, it's my impression that magnesium taurinate is more benefical and so we replaced it with the latter.
We also tried magnesium threonate and magnesium malate. I think these are good forms as well, but I think magnesium N-acetyltaurinate, magnesium taurinate and magnesium bisglycinate are superior.
Magnesium pidolate might be another very good form for seizures, although we have not tried it. One study found that it "was the most efficient in reducing the permeability [of the blood brain barrier] and in enhancing magnesium transport through the barrier." This is important because the blood brain barrier is well known to be impaired in epilepsy:
Magnesium and the blood-brain barrier in vitro: effects on permeability and magnesium transport - PubMed
The blood-brain barrier (BBB) tightly regulates the homeostasis of the central nervous system, and its dysfunction has been described in several neurological disorders. Since magnesium exerts a protective effect in the brain, we assessed whether supraphysiological concentrations of different...
pubmed.ncbi.nlm.nih.gov
Apart from that, magnesium pidolate has been demonstrated to be one of the most effective magnesium forms for preventing seizures in animals (see studies above) and it has been widely and successully used (particularly in Italy and France) for the prevention of migraine and tension headaches in children, which I take as a very good sign because migraine and epilepsy have many things in common and what works for migraines usually also works for seizures.
Magnesium as a preventive treatment for paediatric episodic tension-type headache: results at 1-year follow-up - PubMed
The objective was to confirm the long-term utility of magnesium salts treatment on a group of young patients suffering from episodic tension-type headache (ETTH). The study was carried out at the Outpatient Headache Center at the National Neurological Institute "C. Besta," Milan, Italy, with 45...
pubmed.ncbi.nlm.nih.gov
Last edited: