FoodForeal
Member
Awesome will look tomorrow I think.Got arround that
If anyone wants to buy this book it probably has a lot of good info for $150 lol. The Apex Apicomplexan.
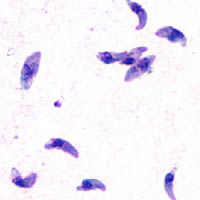
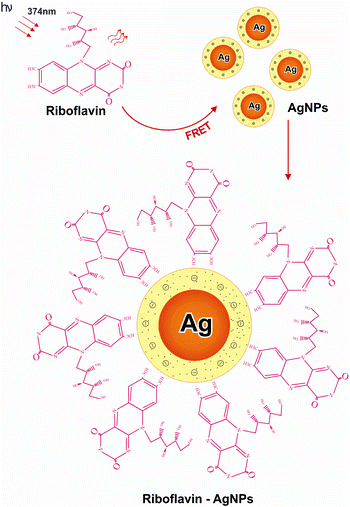
Toxoplasma Gondii
Toxoplasmosis is caused by a one-celled protozoan parasite known as Toxoplasma gondii. In the United States, it is estimated that approximately 30% of cats, the primary carriers, have been infected by T. gondii. Most humans contract toxoplasmosis by eating cyst-contaminated raw or undercooked...
books.google.com
I found the book from a wikipedia citation link on a sentence about the parasitophorous vacuole forming the bradyzoite cyst because I want to know more about how it works but it's behind the paywall: Toxoplasma gondii - Wikipedia
"The cyst wall is formed by the parasitophorous vacuole membrane.[30]:"
Really it's unbelievable how sophisticated it is and how cats are such a great host allowing it to spread to so many different animals all over the world.
Last edited: