Identification of compounds that suppress Toxoplasma gondii tachyzoites and bradyzoites

Identification of compounds that suppress Toxoplasma gondii tachyzoites and bradyzoites - PubMed
Drug treatment for toxoplasmosis is problematic, because current drugs cannot eradicate latent infection with Toxoplasma gondii and can cause bone marrow toxicity. Because latent infection remains after treatment, relapse of infection is a problem in both infections in immunocompromised patients...
 pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
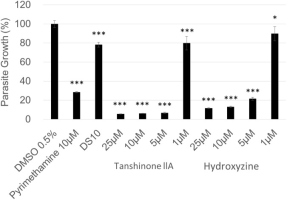
Drug treatment for toxoplasmosis is problematic, because current drugs cannot eradicate latent infection with Toxoplasma gondii and can cause bone marrow toxicity. Because latent infection remains after treatment, relapse of infection is a problem in both infections in immunocompromised patients and in congenitally infected patients. To identify lead compounds for novel drugs against Toxoplasma gondii, we screened a chemical compound library for anti-Toxoplasma activity, host cell cytotoxicity, and effect on bradyzoites. Of 878 compounds screened, 83 demonstrated >90% parasite growth inhibition. After excluding compounds that affected host cell viability, we further characterized two compounds, tanshinone IIA and hydroxyzine, which had IC50 values for parasite growth of 2.5 μM and 1.0 μM, respectively, and had no effect on host cell viability at 25 μM. Both tanshinone IIA and hydroxyzine inhibited parasite replication after invasion and both reduced the number of in vitro-induced bradyzoites, whereas, pyrimethamine, the current therapy, had no effect on bradyzoites. Both tanshinone IIA and hydroxyzine are potent lead compounds for further medicinal chemistry. The method presented for evaluating compounds for bradyzoite efficacy represents a new approach to the development of anti-Toxoplasma drugs to eliminate latency and treat acute infection.
Two old drugs, NVP-AEW541 and GSK-J4, repurposed against the Toxoplasma gondii RH strain

Identification of compounds that suppress Toxoplasma gondii tachyzoites and bradyzoites
Drug treatment for toxoplasmosis is problematic, because current drugs cannot eradicate latent infection with Toxoplasma gondii and can cause bone marrow toxicity. Because latent infection remains after treatment, relapse of infection is a problem in ...
 www.ncbi.nlm.nih.gov
www.ncbi.nlm.nih.gov
Background
Toxoplasma gondii is a zoonotic pathogen that causes toxoplasmosis and leads to serious public health problems in developing countries. However, current clinical therapeutic drugs have some disadvantages, such as serious side effects, a long course of treatment and the emergence of drug-resistant strains. The urgent need to identify novel anti-Toxoplasma drugs has initiated the effective strategy of repurposing well-characterized drugs. As a principled screening for the identification of effective compounds against Toxoplasma gondii, in the current study, a collection of 666 compounds were screened for their ability to significantly inhibit Toxoplasma growth.Hit compounds from 1st screening.
compound | Parasite Inhibition (%)(a) | Host Viability (%)(b) |
|---|---|---|
Bromocriptine | 105 | 85 |
Perphenazine | 104 | 84 |
Mefloquine | 101 | 87 |
Isoconazole | 104 | 101 |
Hydroxyzine | 97 | 101 |
(±)-Terfenadine | 104 | 85 |
Clotrimazol | 99 | 94 |
FLUPHENAZINE | 103 | 83 |
Domperidone | 93 | 94 |
Hycanthone | 97 | 82 |
Propidium Iodide | 91 | 91 |
PENITREM A | 105 | 79 |
Tanshinone IIA | 91 | 83 |
Niguldipine | 103 | 77 |
N-Hydroxy-N2-isobutyl-N2-[(4-methoxyphenyl)sulfonyl]glycinamide | 101 | 98 |
N-{[(2-Methyl-2-propanyl)oxy]carbonyl}glycyl-N-[(2S)-3-methyl-1-oxo-2-butanyl]-L-valinamide | 105 | 106 |
Butein | 96 | 93 |
MC-1293 | 103 | 85 |
Entinostat | 91 | 83 |
TCMDC-125497 | 106 | 82 |
Perospirone | 100 | 96 |
Omeprazole | 92 | 97 |
AM404 | 103 | 100 |
(2Z)-2-(1,3-Benzodioxol-5-yl)-4-(4-methoxyphenyl)-4-oxo-3-(3,4,5-trimethoxybenzyl)-2-butenoic acid | 93 | 85 |
In vitro effects of aqueous extracts of Astragalus membranaceus and Scutellaria baicalensis GEORGI on Toxoplasma gondii
In vitro effects of aqueous extracts of Astragalus membranaceus and Scutellaria baicalensis GEORGI on Toxoplasma gondii | Request PDF
Request PDF | In vitro effects of aqueous extracts of Astragalus membranaceus and Scutellaria baicalensis GEORGI on Toxoplasma gondii | Toxoplasma gondii is a parasite that infects animals and humans worldwide. The standard treatment for toxoplasmosis is limiting due to toxic... | Find, read and...
 www.researchgate.net
www.researchgate.net
Toxoplasma gondii is a parasite that infects animals and humans worldwide. The standard treatment for toxoplasmosis is limiting due to toxic adverse effects, thus there is a need to identify new drugs that are less toxic. Both Astragalus membranaceus and Scutellaria baicalensis GEORGI are popular traditional Chinese herbs widely used for the treatment of various inflammatory diseases in Asia, and we have previously demonstrated that water extracts of A. membranaceus (AmE) and S. baicalensis GEORGI (SbE) have good efficacy in controlling T. gondii replication in mouse models. This study was designed to further evaluate their effects against developing tachyzoites of the RH strain of T. gondii in HeLa cell cultures. AmE, SbE, and TMP-SMX (trimethoprim-sulfamethoxazole) were added into the wells containing both HeLa cells and replicating T. gondii of green fluorescent protein (GFP)-expressing RH tachyzoites. The proliferation and morphous of the tachyzoites were observed, the fluorescence intensity expressed as the fluorescence gray scale value was measured, and the living tachyzoites were counted at different culture times after treatment. The results showed that, compared to untreated controls, parasites treated with either AmE or SbE had significantly decreased intracellular replication at 72, 96, and 120 h after treatment (P < 0.01); while compared to either AmE- or SbE-treated groups, SMX-treated groups had even significantly decreased replication (only a few living parasites were detected) at the above times (P < 0.01). Our data demonstrated that both AmE and SbE had remarkable in vitro activities against T. gondii.
----------------------------------------------------------------------
It seems apparently the parasite infects up to 30% of the population by meaning of consuming foods - most pigs, sheep and goats meat (maybe the milk too) have the parasite cysts.
A non Antibiotic alternative and or combination therapy of Anti-Histamine with anti toxoplasma activity and anti toxoplasma herbals would be quite important.
If Hydroxyzine is highly active against the bug, i wonder if cetirizine is also potent. Also Cyproheptadine has decent inhibitory action. Hydroxyzine has the advantage of killing the bradyzoites not only the tachyzoites. A viable approach is maybe Azithromycin or Doxycycline as main Antibiotic against tachyzoites. Against the bradyzoites stage Hydroxyzine and the herbal TCM medicines Astralagus and Scutellaria Baicalensis, and a diet which incorporates a lot of lutein, which is also active. Also some Lapodin - beta lapachone would round up the kill mix.
Very interesting that some folks had success against serotonergic symptoms with Bromocriptine + Cypro, bromo is highly active and cypro decent.
The connection to schizophrenia is known and schizophrenia has excess serotonin symtoms incl. IBS, so intestinal infection is very likely too.
Toxoplasma is scavening nutrients of its host, a lot of b-vitamins ,so high dose full spectrum is in likely needed too.
I hope this helps a lot of people - i try the herbal mix + Hydroxyzine atm and my ibs is nearly gone, go figure.