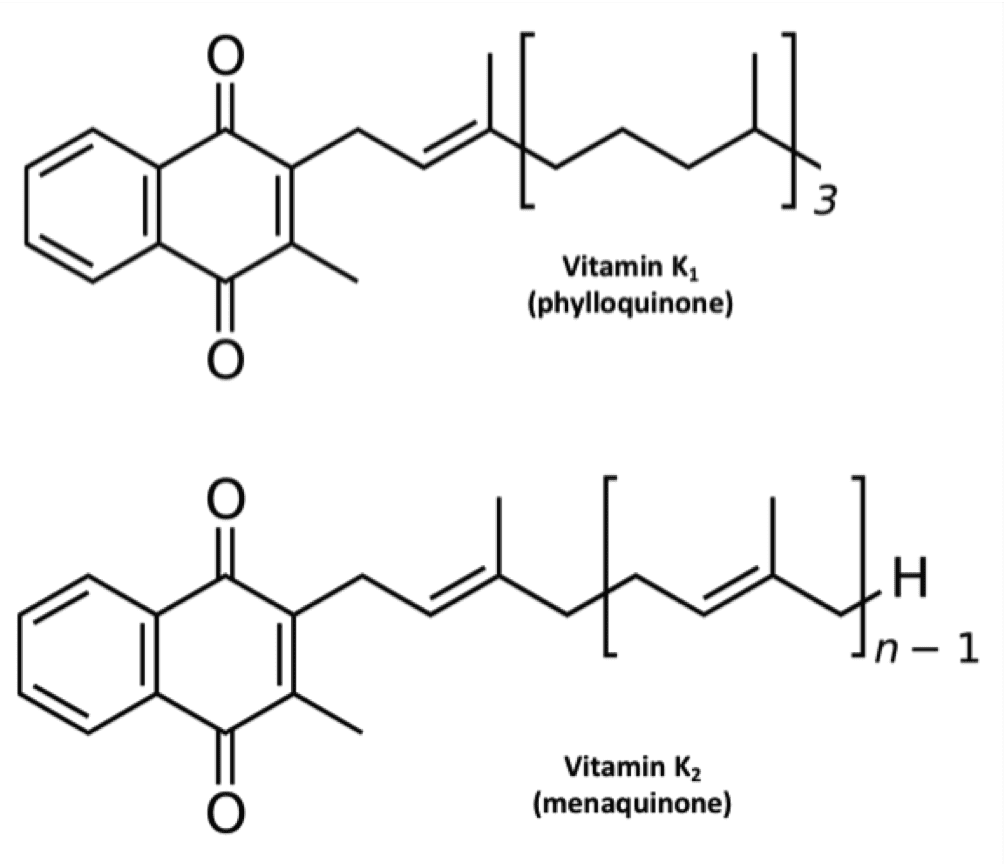
k1 in natto probably come from soy oil,not sure.
Thhere are some good info too: https://raypeatforum.com/community/threads/vitamin-k-in-milk-best-vitamin-k2-source.13148
Thhere are some good info too: https://raypeatforum.com/community/threads/vitamin-k-in-milk-best-vitamin-k2-source.13148