OP
Rinse & rePeat
Member
- Joined
- Mar 10, 2021
- Messages
- 21,516
“Danish study finds superbug C. difficile can jump between pigs and humans, providing evidence of zoonotic spread”
“This alarming discovery suggests that resistance to antibiotics can spread more widely than previously thought, and confirms links in the resistance chain leading from farm animals to humans.”
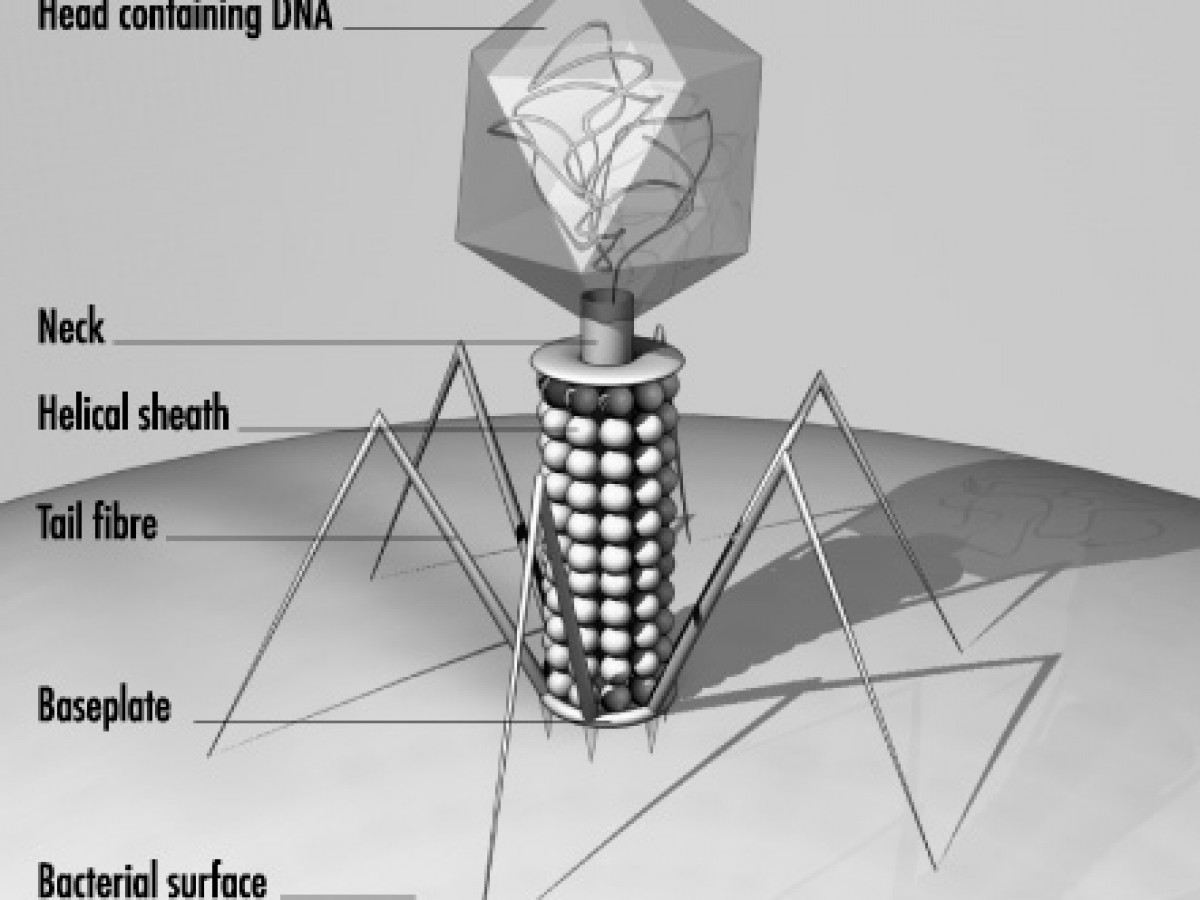
C. difficile is a bacterium that infects the human gut and is resistant to all but three current antibiotics. Some strains contain genes that allow them to produce toxins that can cause damaging inflammation in the gut, leading to life-threatening diarrhoea, mostly in the elderly and hospitalised patients who have been treated with antibiotics.“
“In this study, Danish scientists investigated the prevalence of C. difficile strains in livestock (pigs) and the potential for zoonotic spread of antimicrobial resistance genes by comparing to clinical isolates from Danish hospital patients.
Stool samples were collected from 514 pigs in two batches from farms across Denmark between 2020 and 2021. Batch A included 330 samples from sows, piglets and slaughter pigs from fourteen farms in 2020. The 184 samples in batch B were collected during slaughtering in 2021.
Samples were screened for the presence of C. difficile and genetic sequencing was used to identify whether they harboured toxin and drug resistance genes. Genome sequencing was also used to compare the C. difficile isolates from the pig samples to 934 isolates collected from patients with C. difficile infection over the same period.
Out of 514 pigs samples, 54 had evidence of C. difficile (batch A= 44, batch B=9). Further analyses of 40 samples (batch A=33, batch B=7), found that C. difficile was more common in piglets and sows than slaughter pigs. The authors speculate that this may be due to the difference in age between piglets and adult pigs—with the younger pigs having a microbiota composition that makes them more susceptible to a successful colonization.
In total, thirteen sequence types found in animals matched those found in patient’s stool samples. ST11, an animal-associated strain, was the most common (pig=21, human=270). In sixteen cases, ST11 strains in humans and animals were identical (see table 1 and figure 1 in notes to editors)
All isolates from animals were positive for the toxin genes and ten were also hypervirulent, with an even greater capacity to cause disease.”
“This alarming discovery suggests that resistance to antibiotics can spread more widely than previously thought, and confirms links in the resistance chain leading from farm animals to humans.”
C. difficile is a bacterium that infects the human gut and is resistant to all but three current antibiotics. Some strains contain genes that allow them to produce toxins that can cause damaging inflammation in the gut, leading to life-threatening diarrhoea, mostly in the elderly and hospitalised patients who have been treated with antibiotics.“
“In this study, Danish scientists investigated the prevalence of C. difficile strains in livestock (pigs) and the potential for zoonotic spread of antimicrobial resistance genes by comparing to clinical isolates from Danish hospital patients.
Stool samples were collected from 514 pigs in two batches from farms across Denmark between 2020 and 2021. Batch A included 330 samples from sows, piglets and slaughter pigs from fourteen farms in 2020. The 184 samples in batch B were collected during slaughtering in 2021.
Samples were screened for the presence of C. difficile and genetic sequencing was used to identify whether they harboured toxin and drug resistance genes. Genome sequencing was also used to compare the C. difficile isolates from the pig samples to 934 isolates collected from patients with C. difficile infection over the same period.
Out of 514 pigs samples, 54 had evidence of C. difficile (batch A= 44, batch B=9). Further analyses of 40 samples (batch A=33, batch B=7), found that C. difficile was more common in piglets and sows than slaughter pigs. The authors speculate that this may be due to the difference in age between piglets and adult pigs—with the younger pigs having a microbiota composition that makes them more susceptible to a successful colonization.
In total, thirteen sequence types found in animals matched those found in patient’s stool samples. ST11, an animal-associated strain, was the most common (pig=21, human=270). In sixteen cases, ST11 strains in humans and animals were identical (see table 1 and figure 1 in notes to editors)
All isolates from animals were positive for the toxin genes and ten were also hypervirulent, with an even greater capacity to cause disease.”