BetterCallSaul
Member
- Joined
- Nov 5, 2019
- Messages
- 122
Yes, finasteride. I should have clarified that!")
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.
Click Here if you want to upgrade your account
If you were able to post but cannot do so now, send an email to admin at raypeatforum dot com and include your username and we will fix that right up for you.
Ok... here it is. There's somewhat of a TLDR at the bottom, but I would recommend reading everything... I'm not so sure it would make much sense.
After over a decade of finasteride use and many years spent in recovery, I believe I may know what actually causes the persistent side effects of finasteride use (or PFS). I'll try to explain as clearly as possible, but first I'll start with what I did when I recovered the last time and my process of discovery.
At the time of my last recovery, I was doing quite a few things that I felt could have been responsible for what seemed almost like a spontaneous recovery. It all seemed to happen very quickly... like within the span of a couple months, with some of the most significant changes occurring inside of just a couple weeks.
So, at the time, I had been taking various supplements (namely: riboflavin, niacin, iodine, D3, B12, biotin, l-dopa, and probably a few others). More significantly, I had made some pretty major changes to my diet within only a couple months of complete recovery. So, when I finally did recover, I attributed the recovery to the dietary change because of the many positive changes that had occurred in addition to the recovery. To keep this brief, I'll just say that, eventually, I came to believe that the diet, while still a positive force in my life, was not responsible for my recovery.
So up until about 6 months ago, my list of possible things responsible for my recovery looked about like this:
-dietary changes
- use of l-dopa or high doses of niacin/riboflavin, possibly something else like licorice root that I had been using at the time
- time
I tested the l-dopa and the other stuff and while I experienced similarities with my last recovery, none of this stuff ended up being significant. The only thing left was that I had recovered from PFS because it was simply time.. enough time had passed for whatever was screwed up to reverse itself. At times, I convinced myself of this, but the problem was that only maybe 4 months prior to my recovery, I had used finasteride for maybe around a week and then decided it wasn't worth it and quit. So, while time was still a possibility, I always remained skeptical.
So, being tired of seeing little to no improvement after another 2.5 years of life wasted, I decided to try and exactly retrace every single thing I had done around the time in the exact manner I did it when I recovered... even if it was something I had already done or decided to dismiss as insignificant.
These were the items at the top of my list:
- test the use of one single dose of spironolactone @ 50 mg, which I had used only weeks before recovery
- test a particular type of iodine that I used during the last recovery but hadn't used since
- test the use of the androgen receptor antagonist RU58841 at 40mg/ml twice daily for ~3 weeks
I tested the spironolactone and pretty much nothing happened. I felt odd and a little dehydrated the night I took it and that was essentially it. I'm going to skip past the iodine to the RU58841 and say that I haven't tried this again yet, but it's still on the table because I have a good reason to believe that it could have possibly played a role in the recovery. I'll discuss this later. So, now, I'll get to the iodine. I believe this was actually responsible for the recovery and I'll discuss what has led me to believe this and why I overlooked it for so long to begin with.
During the last recovery, I had been taking iodine very religiously every day along with a bunch of other cofactors which included vitamin C, selenium, riboflavin, and niacin, while also ensuring adequate iron intake. I never felt immediate improvement of anything, nor did I experience a gradual, building improvement of anything. My recovery happened very quickly and suddenly and, because of this, iodine just wasn't on my radar.
So, fast forward to around 6-8 months ago, I began taking high amounts of "nascent" iodine, which, honestly, is probably just sodium or potassium iodide dissolved in glycerin... I really don't know wtf it is because I can't seem to find a straight answer other than the equivalent of "magic" or magnetic charge or some obfuscated pseudoscience. So, I took relatively high amounts for around 2 months... I think I took around 30 drops daily which is the equivalent of around 15 mg. I'm no stranger to this amount of iodine. I've taken higher amounts using 5% lugol's. In fact, probably only a few months prior, I had been taking lugol's. After a month to 2 months of taking the "nascent" iodine, I noticed that I began growing hair on previously barren spots on my hands. At this point, I realized that 5-6 months prior, when I was taking the lugol's iodine, I also grew this hair on my hands. The problem was that I never attributed the hair growth to the iodine and, even worse, 2 months after I quit using lugol's, the hair on my hands fell out again and I still hadn't realized the connection. It wasn't until I tried the experiment with the stupid nascent iodine and saw the hair growth inside of 1.5 months that I finally made the connection. Not coincidentally, I also experienced this increase in hair growth on my hands (and body hair, in general) during my last recovery.
Ok, so at this point, anyone reading this is probably thinking THYROID.. and yes, obviously, that's where this leads, but there's a little more to it and I believe this is important because it offers insight into what PFS might actually be and what causes it. I want to go back in time to when I first began taking finasteride. Over a decade ago, I took the typical 1 mg daily finasteride and it worked incredibly well, but also caused the horrible side effects. At that time, when I quit taking finasteride, it only took maybe 3-4 weeks for my body to make a full recovery and go back to normal. As I continued toying with finasteride over the years to discover what made it work and why it would stop working after only a few weeks to a month or two of use, the time it took to recover from finasteride after discontinuation gradually increased. Eventually it started taking 3-4 months and then seemingly 3-4 years based on the last recovery.
So, I thought that finasteride must be causing some type of long-term damage or epigenetic changes that cause the recovery time to perpetually increase with each subsequent use. What I hadn't considered, however, was that perhaps there was some underlying condition or genetic susceptibility that finasteride will exacerbate, but of which it isn't necessarily the cause. I've had hypothyroid-like symptoms since childhood, but I've never been diagnosed with hypothyroidism because my labwork has never indicated clinical hypothyroidism. I don't really have any thyroid labwork from a time prior to finasteride use, but anyone here that looked at my labwork done during PFS would assume hypothyroidism based off the TSH values. T4 and T3 levels seemed normal and within "range", but ranges don't really mean much to me anymore because the range that's right is what feels good.... not where the average of the population rests.
Anyway I started traversing the clinical and scientific literature for associations between thyroid and 5a reductase, as well as various other things like androgen receptor and 5AR antagonist, androgen receptor and thyroid, thyroid and prolactin, thyroid and gonadotropin releasing hormone.... and many other searches like this. I was trying to piece together a narrative that I was building in my head.. trying to tie all the things I already knew to what I had recently learned about the significance of iodine in my recovery.
At this point, I'm just going to start citing some of the studies and research I read and what I was thinking as I was reading them and what they subsequently led to. So, the first one I have is "Reversible 5α-reductase 2 deficiency in Hypothyroidism":
So, this essentially outlines a few case studies of "severe primary acquired auto-immune hypothyroidism, which show a similar picture of 5α-reductase deficiency". My first thoughts were that there seems to be a sort of "chicken and egg" situation... did the 5AR deficiency cause the hypothyroidism or the other way around? Or is there perhaps some sort of interdependence where either one could cause the other? Either way, they demonstrated that the type 2 5AR (SRD5A2) deficiency was completely reversible following administration of adequate thyroxine. So, great... I've found an association between 5AR deficiency and hypothyroidism. So, now, I know that anyone taking finasteride (or any other potent 5AR antagonist) could be inducing hypothyroidism. But then the question becomes "Well, if finasteride can induce hypothyroidism, then shouldn't that work itself out after discontinuation of fin?". And the answer, at least for most people that don't experience PFS, is probably yes. So, what about those who experience PFS? One thing I think is important to do when dealing with these chicken and egg situations is ask if the relationship between, for example, 5AR and hypothyroidism has any reflexivity in their associations. So, we know that hypothyroidism seems to be able to induce deficiency of SRD5A2 expression, but is it also possible that pharmaceutically induced 5AR deficiency can cause hypothyroidism which can then prevent return of normal 5AR expression?
Here's another study done on rats that seems to corroborate the previously mentioned 3 case studies:
(in case above link doesn't work: www(dot) jbc.org/article/S0021-9258(17)30647-6/pdf )
"Although GH has been shown to exert a positive, stimulatory effect on hepatic 5α-reductase activity when present continuously (Mode et al., 1982), the inability to support full enzyme expression in hypophysectomized rats (Waxman et al., 1989a and this study) led to the proposal that the effects of GH may require mediation by or interaction with other pituitary-dependent factors. The present study validates this hypothesis and establishes that T4, wihch is dependent on pituitary thyroid-stimuating hormone for secretion by the thyroid, can significantly restore hepatic 5α-reductase activity and its mRNA, both in hypophysectomized rats and hypothyroid rats."
Here's an excellent article that reviews the current state of research on the 5α-reductases and their physiological importance:
Of particular interest in this article is section 4.4 Thyroid hormones and androgens crosstalk. Read the whole section, but I'll point out what I find most significant.
They state: "hypothyroidism can decrease androgens, LH, and gonadotropin-releasing hormone levels, (rat: Chiao et al., 1999; Kala et al., 2002; bird: Weng et al., 2007; fish: Swapna et al., 2006), impair testicular development (rat: Wagner et al., 2008; Maran, 2009), induce atrophy of epididymis and seminiferous tubules, decrease sperm number and motility (rat: Anbalagan et al., 2010; bird: Weng et al., 2007; fish: Swapna et al., 2006), and can even lead to a female biased sex ratio (frog: Goleman et al., 2002; fish: Mukhi et al., 2007)".
Much of this is part of the manifestation of PFS, obviously. What I found more interesting, though is that 5AR expression appears to be regulated by a thyroid hormone response element (TRE) which is found within the promoter region of every 5AR isoform:
"This cross-regulation of SRD5αs by TH can be explained by predicted thyroid hormone response element (TRE) in the promoter of each SRD5α isoforms (Flood et al., 2013). However, the functionality of those TREs still remains to be tested to ascertain their direct role in the regulation of SRD5αs."
So, that question I asked earlier about reflexivity... hypothyroidism seems to be able to induce 5AR deficiency (as shown in the case studies as well as the apparent connection between 5AR expression and TREs in the genes encoding for each 5AR isoform), but is there a connection between pharmaceutically-induced 5AR deficiency and hypothyroidism? There appears to be:
"another important aspect in TH regulation is the existing crosstalk with androgens due to the presence of ARE in genes related to THs, such as deiodinases and TH receptors (reviewed by Flood et al., 2013). Indeed, 5α-DHT treatment increases transcription of thyroid receptor β and deiodinase 1 (Campbell and Langois et al., 2018), and FIN treatment impacts expression of TH-related genes such as deiodinase and TH receptors in S. tropicalis (Langois et al., 2010b; Langois et al., 2011)."
So, there are androgen response elements within the genes encoding for deiodinases and thyroid hormone receptors and DHT treatment increases transcription of thyroid receptor β and deiodinase 1. Moreover, treatment of finasteride impacts the expression of these genes. So, what I'm seeing here is not only a classical picture of hypothyroidism (where only thyroid hormones are insufficient), but potentially hypothyroidism on the receptor side. With pharmaceutically-induced 5AR deficiency, low synthesis of DHT can cause an under-expression of the genes for deiodinase 1 (which plays a direct role in deiodinating T4 to the active T3) and for thyroid receptor β. So, if hypothyroidism isn't being induced by lack of thyroid hormones (perhaps you may be supplementing THs?), it can also be induced by lack of thyroid hormone receptor β expression. That hypothyroidism can then cause a sort of catch-22 situation where you don't have 5AR expression (and, thus, no DHT), so you can't express TH receptors properly, and you don't have sufficient thyroid hormone stimulation of tissues, so you can't express 5AR. This is the essence of post-finasteride syndrome in my opinion.
Consequently, anyone who also happens to have a perpetually worsening thyroid condition seems to be far more likely to experience PFS. This, perhaps, explains why some people seem to be profoundly affected long-term by 5AR antagonists and others seem to bounce back just fine after discontinuation. It also explains why, with each subsequent use of finasteride, it took longer for me to recover... because I likely have a perpetually worsening thyroid condition.
BUT WAIT! THERE'S MORE! Don't worry. I'm going to tie all of this together in the end and it should give a nice picture of the etiology of PFS.
So, next, I want to talk about the association of elevated prolactin levels, hypothyroidism, and PFS. Let's start with this study:

Hyperprolactinemia in association with subclinical hypothyroidism
Background: Hyperprolactinemia is the most common endocrine disorder in hypothalamic-pituitary axis and has been reported in variable levels in patients with overt primary hypothyroidism. We decided to determine the prevalence of hyperprolactinemia and ...www.ncbi.nlm.nih.gov
I'm not going to say much about it, but you can read it if you'd like. The study shows "the prevalence of hypothyroidism symptoms in subclinical hypothyroidism on males and females." and "showed the higher prevalence of hyperprolactinemia in subclinical hypothyroidism in female than male, this prevalence was 21.7% and 11.3%, respectively."
I'll include this as well since it's relevant and interesting: "In hypothyroidism patients, TRH is the stimulant factor of rising prolactin level. A previous study suggested that perhaps estrogen caused to increase prolactin response to TRH that caused higher prolactin level in woman than men (22). Meier et al. reported that women before menopause or menopausal women that received estrogen had higher level of prolactin compared to menopausal women without estrogen replacement (21)."
So, the questions I have when I read this are:
- Why does prolactin seem to be elevated in hypothyroidism (and, consequently, why is it elevated in many who suffer from PFS)?
- Assuming the answer to the question above is that prolactin is released in a sort of package along with thyrotropin releasing hormone, is there any other possible reason for the increase in prolactin?
And a follow-up question to those two questions: Is elevated prolactin a side effect... collateral damage?... just a co-secretion along with TRH that needs to be controlled or lowered, or is its presence there to help address a deeper problem? I think, yes...

Effect of prolactin on sodium iodide symporter expression in mouse mammary gland explants - PubMed
Iodide accumulates in milk at a concentration that is more than an order of magnitude higher than the iodide concentration in maternal plasma. In earlier studies from our laboratory, we have shown that prolactin (PRL) enhances iodide accumulation by two- to threefold in cultured mammary tissues...pubmed.ncbi.nlm.nih.gov
This is in mice, so take it for what you will. However, I believe that there is very likely the same or similar mechanism in humans.
"In earlier studies from our laboratory, we have shown that prolactin (PRL) enhances iodide accumulation by two- to threefold in cultured mammary tissues taken from pregnant mice... The lowest PRL concentration that elicited a significant response was 1 ng/ml, and a maximum effect was elicited with PRL concentrations >100 ng/ml. Actinomycin D, cycloheximide, and thiocyanate abolished the PRL effect on NIS accumulation, whereas perchlorate was without effect. These studies suggest that the PRL stimulation of iodide accumulation in milk is mediated, at least in part, by the PRL stimulation of NIS accumulation in mammary gland tissues. These studies further demonstrate that the PRL effect on NIS accumulation occurs via an RNA protein synthesis-dependent mechanism."
So, the sodium iodide symporter (NIS) is a transmembrane protein which is responsible for transporting iodide ion across the cell membrane and concentrating it within the cell. In the mice, prolactin appears to enhance NIS expression. I highlighted thiocyanate since it is a goitrogen when adequate dietary iodine seems to be lacking (just thought it was interesting). So, in a state of hypothyroidism and in PFS, whether clinically diagnosed or subclinical, hyperprolactinemia seems to be present. What are the chances that the elevated prolactin is an effort by the body to increase the expression of NIS to concentrate iodide in response to hypothyroidism? I've not found research on this yet, but I wouldn't be surprised if there's a connection. In case you're not aware of the role of iodine in extrathyroidal tissues, here's a reference:
Molecular Iodine Has Extrathyroidal Effects as an Antioxidant, Differentiator, and Immunomodulator
Most investigations of iodine metabolism in humans and animals have focused on its role in thyroid function. However, considerable evidence indicates that iodine could also be implicated in the physiopathology of other organs. We review the literature ...
There are many tissues, other than breast and thyroid tissue, that express NIS and accumulate iodide. The role iodide/iodine in these tissues is not yet very well understood.
Additionally, I thought I might add that TSH itself also induces expression of NIS:
"TSH stimulation of NIS mRNA and protein expression are mediated by the cAMP pathway in rodent cell lines, Fisher rat thyroid cell line (FRTL)-5 cells (Weiss et al. 1984a, Kogai et al. 1997), PC Cl3 immortalized rat thyroid cells (Trapasso et al. 1999), and human primary thyroid cells (Saito et al. 1997, Kogai et al. 2000a). The upregulation of NIS in response to TSH is at both the transcriptional and the post-translational levels. TSH stimulates the NIS promoter and NIS upstream enhancer (NUE; Endo et al. 1997, Ohmori et al. 1998, Ohno et al. 1999, Taki et al. 2002), increases the half-life of the NIS protein, and stimulates the trafficking of the NIS to the plasma membrane (Riedel et al. 2001)... Since TSH stimulates NIS expression in both human and rodent thyroid cells, the regulatory region(s) for NIS induction by TSH was expected to be in sequences common to human and rat NIS genes."
Ok, I have one more connection to make between prolactin, the androgen receptor, and signaling in the hypothalamus and the pituitary.
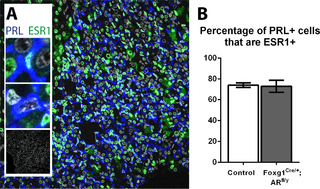
Pituitary Androgen Receptor Signalling Regulates Prolactin but Not Gonadotrophins in the Male Mouse
Production of the androgen testosterone is controlled by a negative feedback loop within the hypothalamic-pituitary-gonadal (HPG) axis. Stimulation of testicular Leydig cells by pituitary luteinising hormone (LH) is under the control of hypothalamic gonadotrophin releasing hormone (GnRH), while...journals.plos.org
In this study they essentially show that ablation of the AR in rat pituitary gland "resulted in no change in circulating testosterone levels, questioning the currently accepted paradigm of testosterone-mediated feedback at the level of the pituitary."
"Further to this observation, in this study we demonstrate that circulating gonadotrophin levels are unaffected by loss of pituitary AR, suggesting androgens do not mediate negative feedback on the HPG axis at the level of the pituitary in males. Instead, we show that pituitary AR is required for repression of prolactin production and release by the male pituitary."
So, androgenic stimulation is required in the pituitary for suppression of prolactin production. Pharmaceutically-induced 5AR deficiency seems like a good way to cause hyperprolactinemia. It would be interesting to know whether people with congenital 5AR deficiency experience elevate levels of prolactin. I've not looked into this, but just a thought.
So, at the level of the pituitary, AR expression doesn't seem to matter with regard to negative regulation of gonadotropins. However, AR may play a role in negative feedback upstream of the pituitary:
"The male HPG axis paradigm is centred on testosterone providing a negative feedback repression at both the hypothalamus (GnRH production) and pituitary (LH production). Our data show no change in circulating LH or testosterone [16] levels when AR is selectively genetically ablated from the male mouse pituitary. One explanation is that AR signalling, though dispensable at the pituitary level is required at the hypothalamic level. Since GnRH-producing neurons do not express AR [35] the level of hypothalamic repression must be upstream of GnRH production, potentially at the level of kisspeptin-producing neurons, which do express AR [36]."
So, why might this matter? Because 5AR antagonists cause AR overexpression:
Five-alpha Reductase Inhibitor Influences Expression of Androgen Receptor and HOXB13 in Human Hyperplastic Prostate Tissue
Objectives Five-alpha reductase inhibitors (5ARIs) are known as chemopreventive agents in...www.scielo.br
"Due to the lower potency of T compared with DHT, 5ARI significantly decreased the total androgen effect (18). In this study, 5ARI significantly increased AR expression, matching the mechanism of hormone-refractory disease as AR overexpression or amplification."
So, if finasteride induces androgen receptor overexpression, and if there exists a negative feedback loop somewhere upstream of hypothalamic regulation, I'm hypothesizing that it's possible that AR overexpression can cause amplified negative feedback, causing hypogonadism. This, however, is probably predicated upon the presence of 5AR expression (perhaps type 1 5AR?) in this region of the brain to help amplify AR signaling. In this regard, I'm not as confident about the connection between AR overexpression and the persistent side effects associated with PFS. If you haven't realized it yet, this is where I believe the androgen receptor antagonist RU58841 could have possibly played a role in my recovery. However, at the moment, I think this is just very unlikely and that my last recovery was due to the iodine and restoring thyroid function which then restored 5AR expression.
I'll try to briefly recap since this was a lot of information:
- 5AR deficiency is able to be reversed in cases of hypothyroidism when thyroxine is administered (in both humans and rats)
- Hypothyroidism can cause hypogonadism
- There are thyroid hormone response elements (TREs) present in the promoter regions of the genes encoding for all isoforms of 5AR, indicating that thyroid hormones play a role in the positive regulation of 5AR expression
- There are androgen response elements present in the genes that encode for thyroid receptor β and deiodinase 1, indicating that androgen signaling plays a role in positive regulation of thyroid receptors and an enzyme that catalyzes the activation of T4 to T3
- PFS appears to be a catch-22 situation where you don't have 5AR expression (and, thus, no DHT), so you can't express TH receptors properly, and you don't have sufficient thyroid hormone stimulation of tissues, so you can't express 5AR
- Hypothyroidism is associated with hyperprolactinemia
- Elevation of prolactin and TSH increases expression of sodium iodide symporter in an effort to increase concentration of iodide within the cell
- Androgen signaling in the pituitary suppresses prolactin secretion
- Finasteride causes AR overexpression
I could probably say a lot more, but I'm tired. At some point, I think it would be nice to make a flow-chart to illustrate the interdependence of these issues.
Wow man. This is a beautiful post. I feel like I should send you money for how insightful and helpful this article is.Ok... here it is. There's somewhat of a TLDR at the bottom, but I would recommend reading everything... I'm not so sure it would make much sense.
After over a decade of finasteride use and many years spent in recovery, I believe I may know what actually causes the persistent side effects of finasteride use (or PFS). I'll try to explain as clearly as possible, but first I'll start with what I did when I recovered the last time and my process of discovery.
At the time of my last recovery, I was doing quite a few things that I felt could have been responsible for what seemed almost like a spontaneous recovery. It all seemed to happen very quickly... like within the span of a couple months, with some of the most significant changes occurring inside of just a couple weeks.
So, at the time, I had been taking various supplements (namely: riboflavin, niacin, iodine, D3, B12, biotin, l-dopa, and probably a few others). More significantly, I had made some pretty major changes to my diet within only a couple months of complete recovery. So, when I finally did recover, I attributed the recovery to the dietary change because of the many positive changes that had occurred in addition to the recovery. To keep this brief, I'll just say that, eventually, I came to believe that the diet, while still a positive force in my life, was not responsible for my recovery.
So up until about 6 months ago, my list of possible things responsible for my recovery looked about like this:
-dietary changes
- use of l-dopa or high doses of niacin/riboflavin, possibly something else like licorice root that I had been using at the time
- time
I tested the l-dopa and the other stuff and while I experienced similarities with my last recovery, none of this stuff ended up being significant. The only thing left was that I had recovered from PFS because it was simply time.. enough time had passed for whatever was screwed up to reverse itself. At times, I convinced myself of this, but the problem was that only maybe 4 months prior to my recovery, I had used finasteride for maybe around a week and then decided it wasn't worth it and quit. So, while time was still a possibility, I always remained skeptical.
So, being tired of seeing little to no improvement after another 2.5 years of life wasted, I decided to try and exactly retrace every single thing I had done around the time in the exact manner I did it when I recovered... even if it was something I had already done or decided to dismiss as insignificant.
These were the items at the top of my list:
- test the use of one single dose of spironolactone @ 50 mg, which I had used only weeks before recovery
- test a particular type of iodine that I used during the last recovery but hadn't used since
- test the use of the androgen receptor antagonist RU58841 at 40mg/ml twice daily for ~3 weeks
I tested the spironolactone and pretty much nothing happened. I felt odd and a little dehydrated the night I took it and that was essentially it. I'm going to skip past the iodine to the RU58841 and say that I haven't tried this again yet, but it's still on the table because I have a good reason to believe that it could have possibly played a role in the recovery. I'll discuss this later. So, now, I'll get to the iodine. I believe this was actually responsible for the recovery and I'll discuss what has led me to believe this and why I overlooked it for so long to begin with.
During the last recovery, I had been taking iodine very religiously every day along with a bunch of other cofactors which included vitamin C, selenium, riboflavin, and niacin, while also ensuring adequate iron intake. I never felt immediate improvement of anything, nor did I experience a gradual, building improvement of anything. My recovery happened very quickly and suddenly and, because of this, iodine just wasn't on my radar.
So, fast forward to around 6-8 months ago, I began taking high amounts of "nascent" iodine, which, honestly, is probably just sodium or potassium iodide dissolved in glycerin... I really don't know wtf it is because I can't seem to find a straight answer other than the equivalent of "magic" or magnetic charge or some obfuscated pseudoscience. So, I took relatively high amounts for around 2 months... I think I took around 30 drops daily which is the equivalent of around 15 mg. I'm no stranger to this amount of iodine. I've taken higher amounts using 5% lugol's. In fact, probably only a few months prior, I had been taking lugol's. After a month to 2 months of taking the "nascent" iodine, I noticed that I began growing hair on previously barren spots on my hands. At this point, I realized that 5-6 months prior, when I was taking the lugol's iodine, I also grew this hair on my hands. The problem was that I never attributed the hair growth to the iodine and, even worse, 2 months after I quit using lugol's, the hair on my hands fell out again and I still hadn't realized the connection. It wasn't until I tried the experiment with the stupid nascent iodine and saw the hair growth inside of 1.5 months that I finally made the connection. Not coincidentally, I also experienced this increase in hair growth on my hands (and body hair, in general) during my last recovery.
Ok, so at this point, anyone reading this is probably thinking THYROID.. and yes, obviously, that's where this leads, but there's a little more to it and I believe this is important because it offers insight into what PFS might actually be and what causes it. I want to go back in time to when I first began taking finasteride. Over a decade ago, I took the typical 1 mg daily finasteride and it worked incredibly well, but also caused the horrible side effects. At that time, when I quit taking finasteride, it only took maybe 3-4 weeks for my body to make a full recovery and go back to normal. As I continued toying with finasteride over the years to discover what made it work and why it would stop working after only a few weeks to a month or two of use, the time it took to recover from finasteride after discontinuation gradually increased. Eventually it started taking 3-4 months and then seemingly 3-4 years based on the last recovery.
So, I thought that finasteride must be causing some type of long-term damage or epigenetic changes that cause the recovery time to perpetually increase with each subsequent use. What I hadn't considered, however, was that perhaps there was some underlying condition or genetic susceptibility that finasteride will exacerbate, but of which it isn't necessarily the cause. I've had hypothyroid-like symptoms since childhood, but I've never been diagnosed with hypothyroidism because my labwork has never indicated clinical hypothyroidism. I don't really have any thyroid labwork from a time prior to finasteride use, but anyone here that looked at my labwork done during PFS would assume hypothyroidism based off the TSH values. T4 and T3 levels seemed normal and within "range", but ranges don't really mean much to me anymore because the range that's right is what feels good.... not where the average of the population rests.
Anyway I started traversing the clinical and scientific literature for associations between thyroid and 5a reductase, as well as various other things like androgen receptor and 5AR antagonist, androgen receptor and thyroid, thyroid and prolactin, thyroid and gonadotropin releasing hormone.... and many other searches like this. I was trying to piece together a narrative that I was building in my head.. trying to tie all the things I already knew to what I had recently learned about the significance of iodine in my recovery.
At this point, I'm just going to start citing some of the studies and research I read and what I was thinking as I was reading them and what they subsequently led to. So, the first one I have is "Reversible 5α-reductase 2 deficiency in Hypothyroidism":
So, this essentially outlines a few case studies of "severe primary acquired auto-immune hypothyroidism, which show a similar picture of 5α-reductase deficiency". My first thoughts were that there seems to be a sort of "chicken and egg" situation... did the 5AR deficiency cause the hypothyroidism or the other way around? Or is there perhaps some sort of interdependence where either one could cause the other? Either way, they demonstrated that the type 2 5AR (SRD5A2) deficiency was completely reversible following administration of adequate thyroxine. So, great... I've found an association between 5AR deficiency and hypothyroidism. So, now, I know that anyone taking finasteride (or any other potent 5AR antagonist) could be inducing hypothyroidism. But then the question becomes "Well, if finasteride can induce hypothyroidism, then shouldn't that work itself out after discontinuation of fin?". And the answer, at least for most people that don't experience PFS, is probably yes. So, what about those who experience PFS? One thing I think is important to do when dealing with these chicken and egg situations is ask if the relationship between, for example, 5AR and hypothyroidism has any reflexivity in their associations. So, we know that hypothyroidism seems to be able to induce deficiency of SRD5A2 expression, but is it also possible that pharmaceutically induced 5AR deficiency can cause hypothyroidism which can then prevent return of normal 5AR expression?
Here's another study done on rats that seems to corroborate the previously mentioned 3 case studies:
(in case above link doesn't work: www(dot) jbc.org/article/S0021-9258(17)30647-6/pdf )
"Although GH has been shown to exert a positive, stimulatory effect on hepatic 5α-reductase activity when present continuously (Mode et al., 1982), the inability to support full enzyme expression in hypophysectomized rats (Waxman et al., 1989a and this study) led to the proposal that the effects of GH may require mediation by or interaction with other pituitary-dependent factors. The present study validates this hypothesis and establishes that T4, wihch is dependent on pituitary thyroid-stimuating hormone for secretion by the thyroid, can significantly restore hepatic 5α-reductase activity and its mRNA, both in hypophysectomized rats and hypothyroid rats."
Here's an excellent article that reviews the current state of research on the 5α-reductases and their physiological importance:
Of particular interest in this article is section 4.4 Thyroid hormones and androgens crosstalk. Read the whole section, but I'll point out what I find most significant.
They state: "hypothyroidism can decrease androgens, LH, and gonadotropin-releasing hormone levels, (rat: Chiao et al., 1999; Kala et al., 2002; bird: Weng et al., 2007; fish: Swapna et al., 2006), impair testicular development (rat: Wagner et al., 2008; Maran, 2009), induce atrophy of epididymis and seminiferous tubules, decrease sperm number and motility (rat: Anbalagan et al., 2010; bird: Weng et al., 2007; fish: Swapna et al., 2006), and can even lead to a female biased sex ratio (frog: Goleman et al., 2002; fish: Mukhi et al., 2007)".
Much of this is part of the manifestation of PFS, obviously. What I found more interesting, though is that 5AR expression appears to be regulated by a thyroid hormone response element (TRE) which is found within the promoter region of every 5AR isoform:
"This cross-regulation of SRD5αs by TH can be explained by predicted thyroid hormone response element (TRE) in the promoter of each SRD5α isoforms (Flood et al., 2013). However, the functionality of those TREs still remains to be tested to ascertain their direct role in the regulation of SRD5αs."
So, that question I asked earlier about reflexivity... hypothyroidism seems to be able to induce 5AR deficiency (as shown in the case studies as well as the apparent connection between 5AR expression and TREs in the genes encoding for each 5AR isoform), but is there a connection between pharmaceutically-induced 5AR deficiency and hypothyroidism? There appears to be:
"another important aspect in TH regulation is the existing crosstalk with androgens due to the presence of ARE in genes related to THs, such as deiodinases and TH receptors (reviewed by Flood et al., 2013). Indeed, 5α-DHT treatment increases transcription of thyroid receptor β and deiodinase 1 (Campbell and Langois et al., 2018), and FIN treatment impacts expression of TH-related genes such as deiodinase and TH receptors in S. tropicalis (Langois et al., 2010b; Langois et al., 2011)."
So, there are androgen response elements within the genes encoding for deiodinases and thyroid hormone receptors and DHT treatment increases transcription of thyroid receptor β and deiodinase 1. Moreover, treatment of finasteride impacts the expression of these genes. So, what I'm seeing here is not only a classical picture of hypothyroidism (where only thyroid hormones are insufficient), but potentially hypothyroidism on the receptor side. With pharmaceutically-induced 5AR deficiency, low synthesis of DHT can cause an under-expression of the genes for deiodinase 1 (which plays a direct role in deiodinating T4 to the active T3) and for thyroid receptor β. So, if hypothyroidism isn't being induced by lack of thyroid hormones (perhaps you may be supplementing THs?), it can also be induced by lack of thyroid hormone receptor β expression. That hypothyroidism can then cause a sort of catch-22 situation where you don't have 5AR expression (and, thus, no DHT), so you can't express TH receptors properly, and you don't have sufficient thyroid hormone stimulation of tissues, so you can't express 5AR. This is the essence of post-finasteride syndrome in my opinion.
Consequently, anyone who also happens to have a perpetually worsening thyroid condition seems to be far more likely to experience PFS. This, perhaps, explains why some people seem to be profoundly affected long-term by 5AR antagonists and others seem to bounce back just fine after discontinuation. It also explains why, with each subsequent use of finasteride, it took longer for me to recover... because I likely have a perpetually worsening thyroid condition.
BUT WAIT! THERE'S MORE! Don't worry. I'm going to tie all of this together in the end and it should give a nice picture of the etiology of PFS.
So, next, I want to talk about the association of elevated prolactin levels, hypothyroidism, and PFS. Let's start with this study:
Hyperprolactinemia in association with subclinical hypothyroidism
Background: Hyperprolactinemia is the most common endocrine disorder in hypothalamic-pituitary axis and has been reported in variable levels in patients with overt primary hypothyroidism. We decided to determine the prevalence of hyperprolactinemia and ...
I'm not going to say much about it, but you can read it if you'd like. The study shows "the prevalence of hypothyroidism symptoms in subclinical hypothyroidism on males and females." and "showed the higher prevalence of hyperprolactinemia in subclinical hypothyroidism in female than male, this prevalence was 21.7% and 11.3%, respectively."
I'll include this as well since it's relevant and interesting: "In hypothyroidism patients, TRH is the stimulant factor of rising prolactin level. A previous study suggested that perhaps estrogen caused to increase prolactin response to TRH that caused higher prolactin level in woman than men (22). Meier et al. reported that women before menopause or menopausal women that received estrogen had higher level of prolactin compared to menopausal women without estrogen replacement (21)."
So, the questions I have when I read this are:
- Why does prolactin seem to be elevated in hypothyroidism (and, consequently, why is it elevated in many who suffer from PFS)?
- Assuming the answer to the question above is that prolactin is released in a sort of package along with thyrotropin releasing hormone, is there any other possible reason for the increase in prolactin?
And a follow-up question to those two questions: Is elevated prolactin a side effect... collateral damage?... just a co-secretion along with TRH that needs to be controlled or lowered, or is its presence there to help address a deeper problem? I think, yes...
Effect of prolactin on sodium iodide symporter expression in mouse mammary gland explants - PubMed
Iodide accumulates in milk at a concentration that is more than an order of magnitude higher than the iodide concentration in maternal plasma. In earlier studies from our laboratory, we have shown that prolactin (PRL) enhances iodide accumulation by two- to threefold in cultured mammary tissues...
This is in mice, so take it for what you will. However, I believe that there is very likely the same or similar mechanism in humans.
"In earlier studies from our laboratory, we have shown that prolactin (PRL) enhances iodide accumulation by two- to threefold in cultured mammary tissues taken from pregnant mice... The lowest PRL concentration that elicited a significant response was 1 ng/ml, and a maximum effect was elicited with PRL concentrations >100 ng/ml. Actinomycin D, cycloheximide, and thiocyanate abolished the PRL effect on NIS accumulation, whereas perchlorate was without effect. These studies suggest that the PRL stimulation of iodide accumulation in milk is mediated, at least in part, by the PRL stimulation of NIS accumulation in mammary gland tissues. These studies further demonstrate that the PRL effect on NIS accumulation occurs via an RNA protein synthesis-dependent mechanism."
So, the sodium iodide symporter (NIS) is a transmembrane protein which is responsible for transporting iodide ion across the cell membrane and concentrating it within the cell. In the mice, prolactin appears to enhance NIS expression. I highlighted thiocyanate since it is a goitrogen when adequate dietary iodine seems to be lacking (just thought it was interesting). So, in a state of hypothyroidism and in PFS, whether clinically diagnosed or subclinical, hyperprolactinemia seems to be present. What are the chances that the elevated prolactin is an effort by the body to increase the expression of NIS to concentrate iodide in response to hypothyroidism? I've not found research on this yet, but I wouldn't be surprised if there's a connection. In case you're not aware of the role of iodine in extrathyroidal tissues, here's a reference:
Molecular Iodine Has Extrathyroidal Effects as an Antioxidant, Differentiator, and Immunomodulator
Most investigations of iodine metabolism in humans and animals have focused on its role in thyroid function. However, considerable evidence indicates that iodine could also be implicated in the physiopathology of other organs. We review the literature ...
There are many tissues, other than breast and thyroid tissue, that express NIS and accumulate iodide. The role iodide/iodine in these tissues is not yet very well understood.
Additionally, I thought I might add that TSH itself also induces expression of NIS:
"TSH stimulation of NIS mRNA and protein expression are mediated by the cAMP pathway in rodent cell lines, Fisher rat thyroid cell line (FRTL)-5 cells (Weiss et al. 1984a, Kogai et al. 1997), PC Cl3 immortalized rat thyroid cells (Trapasso et al. 1999), and human primary thyroid cells (Saito et al. 1997, Kogai et al. 2000a). The upregulation of NIS in response to TSH is at both the transcriptional and the post-translational levels. TSH stimulates the NIS promoter and NIS upstream enhancer (NUE; Endo et al. 1997, Ohmori et al. 1998, Ohno et al. 1999, Taki et al. 2002), increases the half-life of the NIS protein, and stimulates the trafficking of the NIS to the plasma membrane (Riedel et al. 2001)... Since TSH stimulates NIS expression in both human and rodent thyroid cells, the regulatory region(s) for NIS induction by TSH was expected to be in sequences common to human and rat NIS genes."
Ok, I have one more connection to make between prolactin, the androgen receptor, and signaling in the hypothalamus and the pituitary.
Pituitary Androgen Receptor Signalling Regulates Prolactin but Not Gonadotrophins in the Male Mouse
Production of the androgen testosterone is controlled by a negative feedback loop within the hypothalamic-pituitary-gonadal (HPG) axis. Stimulation of testicular Leydig cells by pituitary luteinising hormone (LH) is under the control of hypothalamic gonadotrophin releasing hormone (GnRH), while...
In this study they essentially show that ablation of the AR in rat pituitary gland "resulted in no change in circulating testosterone levels, questioning the currently accepted paradigm of testosterone-mediated feedback at the level of the pituitary."
"Further to this observation, in this study we demonstrate that circulating gonadotrophin levels are unaffected by loss of pituitary AR, suggesting androgens do not mediate negative feedback on the HPG axis at the level of the pituitary in males. Instead, we show that pituitary AR is required for repression of prolactin production and release by the male pituitary."
So, androgenic stimulation is required in the pituitary for suppression of prolactin production. Pharmaceutically-induced 5AR deficiency seems like a good way to cause hyperprolactinemia. It would be interesting to know whether people with congenital 5AR deficiency experience elevate levels of prolactin. I've not looked into this, but just a thought.
So, at the level of the pituitary, AR expression doesn't seem to matter with regard to negative regulation of gonadotropins. However, AR may play a role in negative feedback upstream of the pituitary:
"The male HPG axis paradigm is centred on testosterone providing a negative feedback repression at both the hypothalamus (GnRH production) and pituitary (LH production). Our data show no change in circulating LH or testosterone [16] levels when AR is selectively genetically ablated from the male mouse pituitary. One explanation is that AR signalling, though dispensable at the pituitary level is required at the hypothalamic level. Since GnRH-producing neurons do not express AR [35] the level of hypothalamic repression must be upstream of GnRH production, potentially at the level of kisspeptin-producing neurons, which do express AR [36]."
So, why might this matter? Because 5AR antagonists cause AR overexpression:
Five-alpha Reductase Inhibitor Influences Expression of Androgen Receptor and HOXB13 in Human Hyperplastic Prostate Tissue
Objectives Five-alpha reductase inhibitors (5ARIs) are known as chemopreventive agents in...
"Due to the lower potency of T compared with DHT, 5ARI significantly decreased the total androgen effect (18). In this study, 5ARI significantly increased AR expression, matching the mechanism of hormone-refractory disease as AR overexpression or amplification."
So, if finasteride induces androgen receptor overexpression, and if there exists a negative feedback loop somewhere upstream of hypothalamic regulation, I'm hypothesizing that it's possible that AR overexpression can cause amplified negative feedback, causing hypogonadism. This, however, is probably predicated upon the presence of 5AR expression (perhaps type 1 5AR?) in this region of the brain to help amplify AR signaling. In this regard, I'm not as confident about the connection between AR overexpression and the persistent side effects associated with PFS. If you haven't realized it yet, this is where I believe the androgen receptor antagonist RU58841 could have possibly played a role in my recovery. However, at the moment, I think this is just very unlikely and that my last recovery was due to the iodine and restoring thyroid function which then restored 5AR expression.
I'll try to briefly recap since this was a lot of information:
- 5AR deficiency is able to be reversed in cases of hypothyroidism when thyroxine is administered (in both humans and rats)
- Hypothyroidism can cause hypogonadism
- There are thyroid hormone response elements (TREs) present in the promoter regions of the genes encoding for all isoforms of 5AR, indicating that thyroid hormones play a role in the positive regulation of 5AR expression
- There are androgen response elements present in the genes that encode for thyroid receptor β and deiodinase 1, indicating that androgen signaling plays a role in positive regulation of thyroid receptors and an enzyme that catalyzes the activation of T4 to T3
- PFS appears to be a catch-22 situation where you don't have 5AR expression (and, thus, no DHT), so you can't express TH receptors properly, and you don't have sufficient thyroid hormone stimulation of tissues, so you can't express 5AR
- Hypothyroidism is associated with hyperprolactinemia
- Elevation of prolactin and TSH increases expression of sodium iodide symporter in an effort to increase concentration of iodide within the cell
- Androgen signaling in the pituitary suppresses prolactin secretion
- Finasteride causes AR overexpression
I could probably say a lot more, but I'm tired. At some point, I think it would be nice to make a flow-chart to illustrate the interdependence of these issues.
I should probably add... A really important aspect in my recovery was using DHT along with all of these other things I did. I think finasteride causes epigenetic changes in the body's expression of not only 5AR, but also androgen receptors, aromatase, and estrogen receptors. It also seems to significantly affect dopaminergic function which, specifically, seems to be ameliorated by using DHT. I think the hypothalamus and pituitary functionally change after finasteride due to elevated estrogens and prolactin and the only way to get proper signaling back to restore normal 5AR expression and dopaminergic activity is to provide an environment in the body which is exactly the inverse of what finasteride causes. So, you want to be taking at least 1g/week if transdermal DHT for at least a month, while also taking dopaminergic herbs or l-dopa. You also do not want to use testosterone or hCG or any type of aromatizable androgen or gonadotropins while you're doing this because you want to be shut down and you want low estrogenic and prolactinogenic activity. Once you finish the cycle of DHT (or maybe masteron or proviron) then you can maybe start on something like GnRH/gonadorelin or clomid to encourage testicular steroidogenesis. Hopefully, at that point, your body will have started to adjust epigenetically to the high DHT, high dopamine, low E2, low prolactin environment and your HPTA will be able to function normally instead of being caged due to the suppressive environment caused by having no 5AR expression. The lack of dopamine and high prolactin along with overexpression of the androgen receptor from long term insufficiency of androgenic activity cause a catch-22 type situation where your body can't make the thing whose absence causes the problem to begin with and then this ultimately screws up every other function in the body. The high prolactin, low dopamine, low DHT environment also screws up thyroid function and you'll see a really elevated TSH.Wow man. This is a beautiful post. I feel like I should send you money for how insightful and helpful this article is.
Which herbs did you use for dopamine?If this protocol doesn't work, just do it again until it does. I've taken DHT multiple times in the past couple years and gotten close to feeling like I would be recovered a couple weeks after stopping the DHT, but ultimately drifted back to my previous state. This is very likely due to simply not taking enough for long enough. I should have just purchased more DHT and ran a cycle for a month, but instead took it for maybe 10 days. Iirc, I took it for about 3 weeks when I last recovered and it was probably barely enough to push me over the edge.. I probably got a little lucky. It's also very possible that the l-dopa and other things I had been using at the time helped encourage the changes required to restore proper signaling for healthy, self-sustaining HPTA function and 5AR expression.
Well, you could use mucuna pruriens I guess. Or just use l-dopa. I'm sure there are other herbs that promote synthesis of dopamine or upregulation of dopamine receptors, but the most important thing is really going to be the DHT. Most bodybuilders will probably say that you need to use Testosterone alongside DHT, but, in this particular case, you don't want anything except pure androgenic stimulation with DHT or at least a 5a-reduced steroid. You want testosterone and estradiol to be low for an extended period of time and you want to allow dopaminergic activity to dominate over prolactin as well. So, the mild suppression from the DHT is not something that you want to try and prevent. Allow it to lower T, E2, and prolactin and once you've restored the signaling necessary for maintaining 5AR expression, aromatase expression and steroidogenesis will both increase significantly within a month or two thereafter.Which herbs did you use for dopamine?
Protodioscin seems to cover many of those areas (lowers prolactin, increases LH, increases DHT, increases DHEA, increases dopamine)
It's likely dose dependent. The dose response curve for fin is insane, people are taking way too much. People could retain their hair by taking 1/8 of what the recommended dose is.Yeah, but I know many people who have taken it without significant side effects and with good results so I am not sure if the cons are more significant than the pros.
Right but I don’t think you only have to use DHT as fin lowers multiple other 5AR dependent hormones as shown below. DHT just gets the most attention given the hair aspect. But in theory you should be able to introduce any of these biodentical hormones (not DHT only) that got drastically lowered during fin treatment to trigger the same genetic expressions that occurred pre fin, no (I.e androsterone)If you do this, you also should not expect to feel great while you're on the DHT because you won't. You'll likely feel
- calm (you may feel blunt in terms of emotion, but not bad)
- lowish libido
- you'll probably experience joint pain
- you should experience better digestion and gut motility
- you should experience much better sleep quality.. Sleep will be shorter, but feel longer and dreams should be more vivid
-you may feel an increase in adrenergic activity... So, maybe things like post-prandial or nocturnal tachycardia and heart palpitations
The DHT itself isn't what is going to make you feel good. The DHT is just a tool you're going to use to induce the epigenetic changes necessary to maintain 5AR expression.. To undo the epigenetic changes caused by the typical hormonal state caused by finasteride. If it works, you should start noticing normal function within 3-8 weeks after stopping the DHT. It's possible to maybe speed this up by using something like gonadorelin or maybe clomid after stopping the DHT. You just need the pituitary to start releasing gonadotropins with the changes induced by flooding the body with DHT for an extended period of time. This way, you won't experience suppression due to hypersensitivity of androgen receptors in the pituitary or hypothalamus, since they will have hopefully been down-regulated by the DHT, and, hopefully, the presence of 5AR will discourage suppression by metabolizing androgens away from the aromatase pathway. In the longer term, this will also increase your aromatase expression, which would be a good thing. You need 5AR expression in order to not only regulate estrogenic activity, but also to maintain higher aromatase expression.
I just ordered Andosterone from Idealabs. Would that work? If I use that for a period in the dosage mentioned or slightly higher, say like a mg a day transdermal. My dopamine does feel moderately low, but I do so much to crank it (coffee, sunlight, red light, thiamine, l theanine, etc) Used T3 for the first time today and I felt a pretty positive shift, could be the allo-p I used as well though haha. Do you really think this wouldn’t just slowly heal overtime? Been 3 years for me after a little over 3 months of taking fin.I should probably add... A really important aspect in my recovery was using DHT along with all of these other things I did. I think finasteride causes epigenetic changes in the body's expression of not only 5AR, but also androgen receptors, aromatase, and estrogen receptors. It also seems to significantly affect dopaminergic function which, specifically, seems to be ameliorated by using DHT. I think the hypothalamus and pituitary functionally change after finasteride due to elevated estrogens and prolactin and the only way to get proper signaling back to restore normal 5AR expression and dopaminergic activity is to provide an environment in the body which is exactly the inverse of what finasteride causes. So, you want to be taking at least 1g/week if transdermal DHT for at least a month, while also taking dopaminergic herbs or l-dopa. You also do not want to use testosterone or hCG or any type of aromatizable androgen or gonadotropins while you're doing this because you want to be shut down and you want low estrogenic and prolactinogenic activity. Once you finish the cycle of DHT (or maybe masteron or proviron) then you can maybe start on something like GnRH/gonadorelin or clomid to encourage testicular steroidogenesis. Hopefully, at that point, your body will have started to adjust epigenetically to the high DHT, high dopamine, low E2, low prolactin environment and your HPTA will be able to function normally instead of being caged due to the suppressive environment caused by having no 5AR expression. The lack of dopamine and high prolactin along with overexpression of the androgen receptor from long term insufficiency of androgenic activity cause a catch-22 type situation where your body can't make the thing whose absence causes the problem to begin with and then this ultimately screws up every other function in the body. The high prolactin, low dopamine, low DHT environment also screws up thyroid function and you'll see a really elevated TSH.
Also I gotta say I genuinely appreciate you man. Your article gave me a lot of hope and clarity. If you have a Zelle account I would love to send you 20 bucks just for taking the time to help.I just ordered Andosterone from Idealabs. Would that work? If I use that for a period in the dosage mentioned or slightly higher, say like a mg a day transdermal. My dopamine does feel moderately low, but I do so much to crank it (coffee, sunlight, red light, thiamine, l theanine, etc) Used T3 for the first time today and I felt a pretty positive shift, could be the allo-p I used as well though haha. Do you really think this wouldn’t just slowly heal overtime? Been 3 years for me after a little over 3 months of taking fin.
Ok sorry I totally misread you said a gram a week. Holy ***t. Kinda scared of doing shutdown, what does it feel like? Additionally if my symptoms are not absolutely awful, wake up with morning wood sometimes, no difficulty with sexual function at all, libido a tad low. Mostly worried about depression and anxiety, but to be honest I can’t remember if I always felt this way ya know. Will blasting dht make me freak out? Because I just can’t have like an emotional breakdown or crazy anger. Also where does one get dht if andosterone wouldn’t work.If you do this, you also should not expect to feel great while you're on the DHT because you won't. You'll likely feel
- calm (you may feel blunt in terms of emotion, but not bad)
- lowish libido
- you'll probably experience joint pain
- you should experience better digestion and gut motility
- you should experience much better sleep quality.. Sleep will be shorter, but feel longer and dreams should be more vivid
-you may feel an increase in adrenergic activity... So, maybe things like post-prandial or nocturnal tachycardia and heart palpitations
The DHT itself isn't what is going to make you feel good. The DHT is just a tool you're going to use to induce the epigenetic changes necessary to maintain 5AR expression.. To undo the epigenetic changes caused by the typical hormonal state caused by finasteride. If it works, you should start noticing normal function within 3-8 weeks after stopping the DHT. It's possible to maybe speed this up by using something like gonadorelin or maybe clomid after stopping the DHT. You just need the pituitary to start releasing gonadotropins with the changes induced by flooding the body with DHT for an extended period of time. This way, you won't experience suppression due to hypersensitivity of androgen receptors in the pituitary or hypothalamus, since they will have hopefully been down-regulated by the DHT, and, hopefully, the presence of 5AR will discourage suppression by metabolizing androgens away from the aromatase pathway. In the longer term, this will also increase your aromatase expression, which would be a good thing. You need 5AR expression in order to not only regulate estrogenic activity, but also to maintain higher aromatase expression.
I know this, but there is very little research on how 5AR expression is regulated and I've already recovered from PFS from using DHT. There is at least research that indicates that 5AR is partially regulated by a feed-forward loop in which the DHT synthesized via the enzyme positively regulates its expression. We also know that finasteride causes androgen receptor overexpression and changes in dopaminergic function. So, by flooding the body with DHT for a sustained period of time, you have the ability to undo some of the epigenetic changes caused by fin and down-regulate androgen receptor expression. The DHT will also keep pituitary function somewhat suppressed as well as prolactin secretion, giving your body a chance to adjust to low estrogenic activity and low prolactin and increased dopaminergic function. Doing all of this while supplementing for good thyroid function and metabolic health will act as training wheels for the body to start functioning normally again and restoring proper signaling to maintain proper expression of 5AR and other steroidogenic enzymes as well as steroid receptors. Then you get rid of the training wheels and encourage the body to stand on its own. If its doesn't work and you regress for some reason, then you do it again until it does. I probably won't need to do it more than once, though. The only reason it didn't work the last couple times is because I simply didn't use it long enough. 10 days isn't long enough. I actually used it for 3 weeks when I recovered before.Right but I don’t think you only have to use DHT as fin lowers multiple other 5AR dependent hormones as shown below. DHT just gets the most attention given the hair aspect. But in theory you should be able to introduce any of these biodentical hormones (not DHT only) that got drastically lowered during fin treatment to trigger the same genetic expressions that occurred pre fin, no (I.e androsterone)
Ok so your protocol was basically ~100mg of topical DHT per day? Was it in dmso and did you split up the doses and any specific application site?I know this, but there is very little research on how 5AR expression is regulated and I've already recovered from PFS from using DHT. There is at least research that indicates that 5AR is partially regulated by a feed-forward loop in which the DHT synthesized via the enzyme positively regulates its expression. We also know that finasteride causes androgen receptor overexpression and changes in dopaminergic function. So, by flooding the body with DHT for a sustained period of time, you have the ability to undo some of the epigenetic changes caused by fin and down-regulate androgen receptor expression. The DHT will also keep pituitary function somewhat suppressed as well as prolactin secretion, giving your body a chance to adjust to low estrogenic activity and low prolactin and increased dopaminergic function. Doing all of this while supplementing for good thyroid function and metabolic health will act as training wheels for the body to start functioning normally again and restoring proper signaling to maintain proper expression of 5AR and other steroidogenic enzymes as well as steroid receptors. Then you get rid of the training wheels and encourage the body to stand on its own. If its doesn't work and you regress for some reason, then you do it again until it does. I probably won't need to do it more than once, though. The only reason it didn't work the last couple times is because I simply didn't use it long enough. 10 days isn't long enough. I actually used it for 3 weeks when I recovered before.
There's no reason for me to fool around with other 5a-reduced steroids that are going to be far more expensive than DHT (some, maybe not even realistically accessible) and may ultimately do nothing for me when I already know that DHT works.
I actually used Andractim. I managed to get a few tubes in 2017 and didn't really use it until mid to late 2018. Used a half a tube per week and an 80 g tube of Andractim contains 2 g of DHT. So, I would maybe shoot for around 150 mg per day.Ok so your protocol was basically ~100mg of topical DHT per day? Was it in dmso and did you split up the doses and any specific application site?
Did you use iodine with it or topical DHT only with pro dopamine herbs?
Actually what I'm doing now. Have done 2 cycles of proviron and now doing nolvadex.I should probably add... A really important aspect in my recovery was using DHT along with all of these other things I did. I think finasteride causes epigenetic changes in the body's expression of not only 5AR, but also androgen receptors, aromatase, and estrogen receptors. It also seems to significantly affect dopaminergic function which, specifically, seems to be ameliorated by using DHT. I think the hypothalamus and pituitary functionally change after finasteride due to elevated estrogens and prolactin and the only way to get proper signaling back to restore normal 5AR expression and dopaminergic activity is to provide an environment in the body which is exactly the inverse of what finasteride causes. So, you want to be taking at least 1g/week if transdermal DHT for at least a month, while also taking dopaminergic herbs or l-dopa. You also do not want to use testosterone or hCG or any type of aromatizable androgen or gonadotropins while you're doing this because you want to be shut down and you want low estrogenic and prolactinogenic activity. Once you finish the cycle of DHT (or maybe masteron or proviron) then you can maybe start on something like GnRH/gonadorelin or clomid to encourage testicular steroidogenesis. Hopefully, at that point, your body will have started to adjust epigenetically to the high DHT, high dopamine, low E2, low prolactin environment and your HPTA will be able to function normally instead of being caged due to the suppressive environment caused by having no 5AR expression. The lack of dopamine and high prolactin along with overexpression of the androgen receptor from long term insufficiency of androgenic activity cause a catch-22 type situation where your body can't make the thing whose absence causes the problem to begin with and then this ultimately screws up every other function in the body. The high prolactin, low dopamine, low DHT environment also screws up thyroid function and you'll see a really elevated TSH.
That's a good sign. I have pretty much zero ability to express emotion or feel drive and it's horrible.. There's no way to vent from trauma.Also a couple of weeks after quitting my last cycle of proviron I cried, was years and years ago that I did.
You probably won't get the libido until full recovery is made. The proviron will make libido lower due to the mild suppression and the anti-estrogenic effects of 5a-reduced androgens. Once 5AR expression fully returns and is self-sustaining, though, aromatase expression will also increase shortly after and this is when the libido will return.But didn't feel any different with libido, etc.
Hope so bro, will keep you guys updated.That's a good sign. I have pretty much zero ability to express emotion or feel drive and it's horrible.. There's no way to vent from trauma.
You probably won't get the libido until full recovery is made. The proviron will make libido lower due to the mild suppression and the anti-estrogenic effects of 5a-reduced androgens. Once 5AR expression fully returns and is self-sustaining, though, aromatase expression will also increase shortly after and this is when the libido will return.
There are reports of oral DHT working on meso RX but the bioavailability is much lower and you have to dose frequently.Hope so bro, will keep you guys updated.
But transdermal DHT like you're doing is much better than proviron imo. Proviron has very low bioavailibilty. Also read some anecdotal stuff about guys not feeling anything form oral DHT but they did from transdermal.
What site on the body were you applying it the DHT gel and just one application per day?I actually used Andractim. I managed to get a few tubes in 2017 and didn't really use it until mid to late 2018. Used a half a tube per week and an 80 g tube of Andractim contains 2 g of DHT. So, I would maybe shoot for around 150 mg per day.
At the time I was actually doing quite a lot of things. I was taking iodine, vitamin c, selenium, riboflavin, niacin, D3, B12, I was taking ashwaghanda for a few weeks, l-dopa, and I also ate pretty much exclusively raw fruits, leafy greens, vegetables, and sprouts of various types.. Lots of ginger and turmeric root as well. However, while the diet makes me feel pretty great, I don't think it's relevant in the recovery. I would have liked for it to be, but I think my struggle for the past few years has been pretty conclusive that my diet alone wasn't enough to fix this problem and that the DHT played an essential role in my recovery.
There were a lot of things that happened when I took the DHT that I didn't realize were actually the result of the DHT until more recently when I used it again. I made assumptions that my dietary change caused most of the positive changes. For example, sleep quality was significantly better and falling asleep was very quick. I slept less, but it felt like I was sleeping significantly longer and I also had quite vivid and clear dreams. I also had significantly better digestion and gut motility. However, I attributed these things to the dietary change rather than the DHT and the change in 5AR expression that was occurring.
I also experienced some really nasty side effects from the sudden changes in 5AR expression that occurred. I had very sharp stabbing heart pains that I had falsely attributed to a topical androgen receptor antagonist I was using around the same time. I now know that this effect was not caused by that drug because it had recently occurred again. It is simply the result of a sudden change in 5AR expression when the body has epigenetically adapted to a state of existence without 5AR. The body makes certain steroids at a particular rate for various functions. When you suddenly increase the metabolism of those steroids by 5AR, you no longer have enough of them to do the job they're intended to do and it takes awhile for the body to respond to these changes and upregulate steroidogenesis as well as various other epigenetic changes that must occur due to having an increase in 5a-reduced steroids. So, I had very serious issues with fluid and mineral dysregulation likely because of the rapid metabolism of cortisol and aldosterone to their 5a-reduced derivatives. I had hypokalemia and severe dehydration for weeks along with severe stabbing heart pain and numbness in my left arm. I went to the hospital a number of times because it was serious enough that thought I might not live. I also had complete gastrointestinal paralysis and zero gut motility. I had no way to digest food and no way to get it out either. This all came on very quickly and I was not prepared for it. It was also like 10x worse than what I experienced the last time I recovered, so I wasn't expecting it to be this bad. I was expecting the heart pain and some minor digestive issues, but nothing this bad. The issues were probably compounded by mild hypogonadism and I probably should have taken some clomiphene citrate in retrospect. Things are significantly better now after 2 months, though. It's actually possible that I may not even need the DHT by the time it gets to me, but I ordered it a week ago and I'll likely use it when it arrives unless things get significantly better very quickly.