Cliff Myles
Member
Thanks for the information, Cliff. I'm wondering if you've come across Protocel which has been spreading through word of mouth among the cancer community. The ingredients include rhodizonic acid and it seems to work along the same principles as using quinones to catalyse reactions.
"INGREDIENTS: Protocel’s ingredients are a propriety blend of Tetrahydroxyquinone, Rhodizonic Acid, Sodium, Potassium, Croconic Acid, Triquinoyl, Pyrocatechol, Leuconic Acid, mineral and trace elements including Copper."
I don't have cancer but I tried a few doses two years ago (because it's reputed to be non-toxic and many have taken it for preventive purposes) and it increased my metabolism greatly. I've been researching to understand how it did it's job ever since. The people taking Protocel don't seem to understand just how it actually works (the explanations used are metaphorical rather than technical) but the use of quinones makes me wonder if it follows the same concept.
Here's a blog from one of the stage 4 survivors who used Protocel Beating Cancer Without Breaking a Sweat
Again, not much information on HOW it works other than that it did something good for her.
@Peatfit: No, Koch's reagents have been around since the 1920's
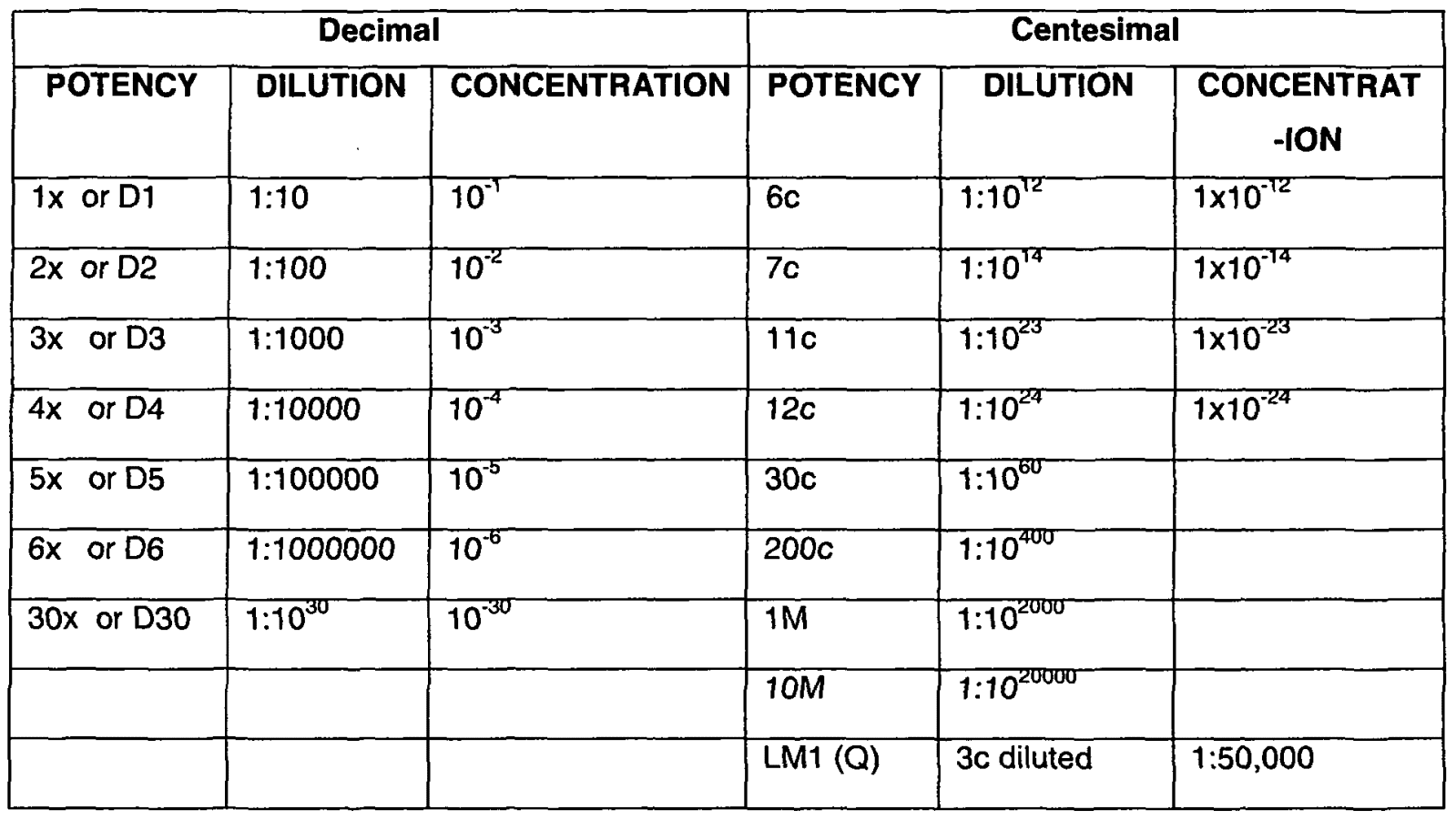
It would be interesting to see what the proportions of the ingredients of Protocel are, and in what dilution.
Koch's reagents were one part per trillion in sterile water, which seems ridiculously small, but you have to fully understand the workings of homeopathy.
This 1/trillion dilution is the main reason the medical profession labeled him a fraud. Very few doctors back then understood homeopathic principles.
Sodium and potassium would have interfered with Koch's reagents, as Reinstorff unsuccessfully tried to develop them into an isotonic solution in order that they might be injected IM or SC without the pain experienced with normal sterile H2O with which theses are normally prepared.
Interesting link, thanks.
@burtlancast Quote:
Daniel Haley has 30 pages on Koch in his splendid book "Politics in healing" where he pretty much demolishes AMA's fairytale.
"They defentely aren't allowed, i'm afraid.
They aren't taught in medical universities; so, any doctor prescribing them is playing with fire."
You got that right, in USA at least... - they would lose their license in a heartbeat !
http://politicsinhealing.com/Dan_Haley-Chap_1.PDF
Politics In Healing: Cures for Cancer banned in USA for political reasons. - 05/01/16
http://www.encognitive.com/files/cc-10 cancer cures that worked.pdf
- CM
Last edited:
")