GorillaHead
Member
I am starting to think Uc is a sugar issue
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.
Click Here if you want to upgrade your account
If you were able to post but cannot do so now, send an email to admin at raypeatforum dot com and include your username and we will fix that right up for you.
Amazing! Thank youNOW brand. It would be my go to. Extraordinary results.

That was going to be my next question to @ecstatichamsterThe capsules or? How much, mixed in how much what? Water?
the study used liquid E from NOW. Just put it into an enema thingie and squirt it up there, hold for 15 minutes.That was going to be my next question to @ecstatichamster

 www.ncbi.nlm.nih.gov
www.ncbi.nlm.nih.gov
8000 IU of alpha tocopherol - that's a huge amount!Rectal administration of d-alpha tocopherol for active ulcerative colitis: A preliminary report
AIM: To investigate the anti-oxidant and anti-neutrophil recruitment effects of rectal d-alpha (d-α) tocopherol administration on mild and moderately active ulcerative colitis (UC).METHODS: Fifteen patients with mild and moderately active ulcerative ...
This is fuccking brilliant thanks , makes perfect senseIBD is constantly labeled as an autoimmune disease but it is not an autoimmune disease but a chronic inflammation due to the immune system attacking itself.
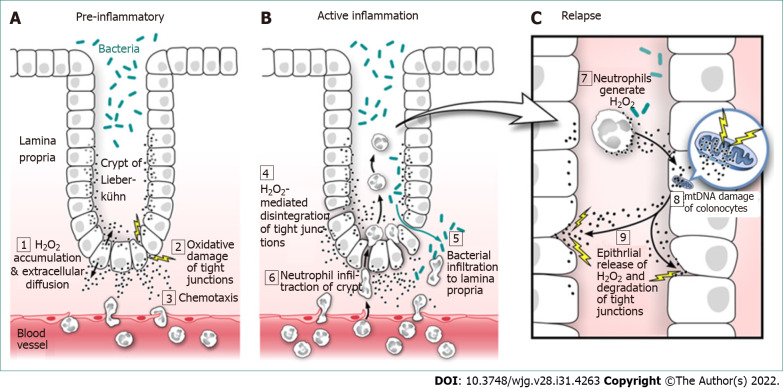
Dr. Jay Pravda claims to have found the cure for Ulcerative Colitis.
h2o2 = permeable from cells (colonic or lower small intestine)
h2o2 = chemotaxic with neutrophils (or in other words , amazingly neutrophils follow hydrogen peroxides trail Chemotaxis - Wikipedia)
mitochondrial DNA damage -> disrupts electron flow in the electron transport chain -> the electrons leak -> combine with oxygen > hydrogen peroxide
& mice lacking GPx develop colitis" GPx2, a gastrointestinal-specific form of GPx [36], which is closely associated with H2O2 metabolism, and whose gene expression is downregulated in several experimental models of UC "
H4R is expressed in the gut mucosa by mucosal immune cells.
Elevated mucosal histamine as well as N-methylhistamine metabolite excretion correlate well with patient disease activity.13, 20, 21, 22
So for a stack / replacements 1. NAC 400mg x2 daily might be able to replace the RD-LA (but would prefer something else if i can find it due to cysteine raising)things mentioned to get / find alternatives to:
* RD-LA orally is the #1 if you can find it , 300mg x2 daily = 85% remission in <8 weeks along with the enema:
. mesalamine 3g [lowers inflammation specific to colonic mucosa]
. budespride 5mg [corticosteroid that inhibits neutrophil infiltration to colon]
. cromolyn sodium 100mg [mast cell stabilizer that prevents release of histamine in the gut]
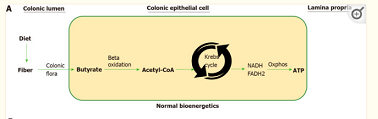
. sodium butyrate 1.7g
* things that increase cellular glutathione, in the colon / intestine (reduces h2o2 to water, helps repair mitochondrial dna -> lower h2o2 production)
(RD-LA increases cellular gluthatione but is not commercially available)
* intracellular antioxidants
* things that help mitochondrial DNA mtDNA repair
* Vitamin B5
* Butyrate
*inhibit gut mast cells / reduce histamine in gut
(specifically H4 antagonists work
*increase NADPH for GSH glutathione recycling
* reduce homocystine (inhibits GPx. take folate? maybe taurine?)
* stuff that increases nuclear factor E2 related factor 2? sulforaphane?
and is backed in ulcerative colitis orally by a case report about 2 women who gained benefit within a couple weeks of higher doseIn vivo bromelain treatment generated a 50-85% reduction in neutrophil migration in 3 different murine models of leukocyte migration into the inflamed peritoneal cavity.
(desloratadine is metabolised from loratadine) and typically low in side effects ,Weller and Maurer report that the H1 antagonist desloratadine possesses mast cell-stabilizing properties when challenged in an IgE-dependent or -independent fashion. Thus, desloratadine provides benefits that are independent of H1 receptor binding and based on mast cell stabilization.
shRNA-induced inhibition of the main transport systems for Cys (ASC1) and cystine (xCT) shows that metastatic activity in NAC-treated mice decreases by approx. 50% if the cystine uptake is inhibited; whereas the inhibition of the Cys uptake does not significantly affect the effect of NAC
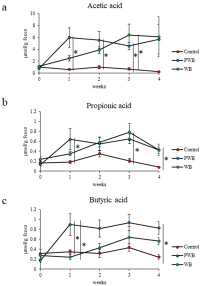
mice in vivo study:The Effects of Intact Cereal Grain Fibers, Including Wheat Bran on the Gut Microbiota Composition of Healthy Adults: A Systematic Review
Thirty-nine of the forty-two studies demonstrated an increase in microbiota diversity and/or abundance following intact cereal fiber consumption, with effects apparent from 24 h to 52 weeks. Increases in wheat fiber as low as 6–8 g were sufficient to generate significant effects
" Of the diet treatments that we examined, the WB-enriched diet continuously produced the highest concentrations of total SCFAs, including butyrate"
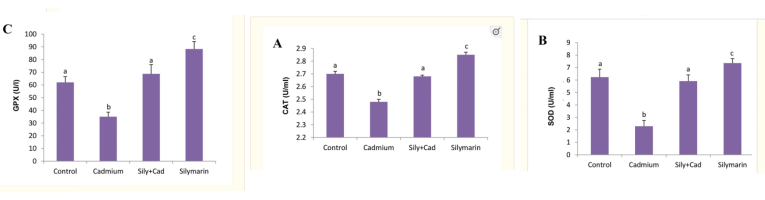
oral consumption of silibinin was associated with a significant increase in both glutathione S-transferase (GST) and quinone reductase (QR) activities in liver, lung, stomach, skin and small bowel in a dose- and time-dependent manner
(effect rose day to day into 14 days, was still rising - so may have continued even more than 2x at 500mgIn the case of GST activity, compared with vehicle-treated controls, treatment with 100 and 200 mg/kg doses of silibinin for 3, 7 and 15 days resulted in 8–110 and 10–140% increases ( P < 0.1–0.001, Student's t -test) in enzyme activity. The observed increase in GST activity was maximum in small bowel at both the doses employed in the study and accounted for the 110 and 140% increases
& a great #6 for the h2o2 (or #1 as might be able to replace NAC without generating cysteine)
Milk thistle (standardized extract)
Silymarin extract of milk thistle , product standardized to high silymarin or silibinin %
www.ncbi.nlm.nih.gov
Also maybe use oat bran instead?@cs3000 super interesting stuff. About the wheat bran, do you think it needs to be cooked, or okay to add as is to smoothies?
@cs3000 super interesting stuff. About the wheat bran, do you think it needs to be cooked, or okay to add as is to smoothies?
havent noticed negatives from eating it uncooked ,Also maybe use oat bran instead?
virus replication silymarin-mediated inhibition of influenza replication occurred through inhibition of late mRNA synthesis. However, whether or not silymarin could modulate other phases of the influenza life cycle was not investigated
Silymarin exhibited anti-influenza A/PR/8/34 virus activity of 98% with no cytotoxicity at the concentration of 100 μg/ml reducing the formation of a visible CPE
(but peak human blood concentration is ng at usual doses, not micrograms)
i think the effect scales with amount of bran fiber eaten. but too much fiber might lower cholesterol & bile acids (idk if that effect is in the small intestine or if its just lower down?)Protective activity of butyrate on hydrogen peroxide-induced DNA damage in isolated human colonocytes and HT29 tumour cells
Pre-incubation of the cells with physiological concentrations of butyrate (6.25 and 12.5 mM) reduced H2O2 (15 μM) induced damage by 33 and 51% in human colonocytes, 45 and 75% in HT29 and 30 and 80% in HT29 19A, respectively.
It should be stressed that butyrate and SCFA mixtures were used at concentrations and relative ratios thought to be physiological in the colon lumen (29
Hi there I would love your thoughts on this very short video especially from the 7.7 minute time.havent noticed negatives from eating it uncooked ,
wheat bran is more effective i think . e.g in the human study when they added 6g oat bran fiber to 6g wheat bran fiber the butyrate effect was the same vs just 6g wheat bran fiber
been taking 250mg-500mg silymarin . no negative effect on mood seems well tolerated so far. the higher folate / b5 doses idk about
Silymarin inhibits T cells potently at physiological concentrations ,
but the compounds have direct antiviral activity so it balances out
hepatitis C Multiple effects of silymarin on the hepatitis C virus lifecycle - Enlighten Publications Silymarin had antiviral effects against hepatitis C virus cell culture (HCVcc) infection that included inhibition of virus entry, RNA and protein expression, and infectious virus production. Silymarin also blocked cell-to-cell spread of virus.
inhibits influenza
"Finally, in vivo oral administration of S0 and S3 not only increased the survival rate in mice infected with a lethal dose of IAV, but also decreased the viral titers in their lungs [23]. Interestingly, this finding is compatible with the accumulation of free silibinin in lung after oral administration that others and we have observed [15,24]. These results, together, point to a prominent role of silymarin as a potent IAV inhibitor."
* net benefit against viral infections in vivo Identification of 23-(S)-2-Amino-3-Phenylpropanoyl-Silybin as an Antiviral Agent for Influenza A Virus Infection In Vitro and In Vivo
s0 = silybin , s1-s5 are the derivatives
25mg/kg , 125mg-150mg silybin, gives +40% survival vs 0% controls in flu challenge. lower virus titer in lungs -
"The mice treated with the 25-mg/kg/day dose of S3 had at least a 100-fold decrease in virus titers in their lungs"
View attachment 49439
also the vitamin b5 raises glutathione peroxidase & reduced glutathione so dual effect with the increased gut energy Effects of dietary pantothenic acid on growth, antioxidant ability and innate immune response in juvenile black carp (might lower GST but the silymarin takes care of that) Curative role of pantothenic acid in brain damage of gamma irradiated rats
& butyrate reduces h2o2 damage in colon cells (& cancer cells , but other mechanisms exist so butyrate is anti-cancer in the colon Sodium Butyrate Selectively Kills Cancer Cells and Inhibits Migration in Colorectal Cancer by Targeting Thioredoxin-1
i think the effect scales with amount of bran fiber eaten. but too much fiber might lower cholesterol & bile acids (idk if that effect is in the small intestine or if its just lower down?)
hi. in the butyrate h2o2 study they used doses that can be found in the colon, and it protected cells decent against h2o2 damage,@cs3000
Hi there I would love your thoughts on this very short video especially from the 7.7 minute time.
He speaks to any vinegar Neutralised by Potassium bicarbonate being A short change fatty acid Going directly into the mitochondria without the pathways that butyrate have to overcome .
He claims vinegar does a better job than actual butyrate.
www.ncbi.nlm.nih.gov
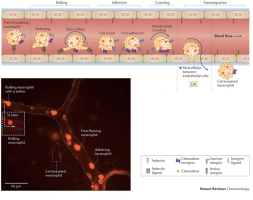
Using the in vivo rat model, we have shown that dietary copper deficiency causes an accumulation of neutrophils in the lung micro vasculature that is 3–4 times greater than that seen in control rats.
The current study was designed to determine whether a diet deficient in copper promotes neutrophil chemoattraction within the lung vasculature or if inadequate copper alters the mechanical properties of the neutrophil, thus restricting passage through the capillary bed
In addition to chemoattraction, neutrophil deformability is a key factor in determining whether neutrophils pass through the lung microvasculature or become lodged in the smallest vessels
copper-deficient neutrophils are less deformable (Fig. 2) and, therefore, are less likely to readily pass through the lung microcirculation
In vitro studies have shown that neutrophils from copper deficient rats pass more readily through endothelial cell monolayers (2, 3), migrate farther in response to IL-8 (3), adhere more to P-selectin (3), and express more CD11b (3) than copper-adequate controls
These results clearly correlate with the decreased deformability of the copper-deficient neutrophils seen in our study (Fig. 2) and suggest a proinflammatory activation of neutrophils in copper-deficient rats
The shape changes also suggest the occurrence of cytoskeletal remodeling, which is required for neutrophils to migrate to the borders of endothelial cells (17) and may account for the greater extravasation of copper-deficient neutrophils through endothelial cell monolayers
In summary, the current study addresses two possible mechanisms for the greater accumulation of neutrophils that occurs in the copper-deficient rat lung. The results
demonstrate that although the inflammatory response in copper-deficient rat lung is exaggerated (4), there is no increase in the production of the chemokine MIP-2 in the absence of an inflammatory stimulus (Fig. 1). The results also demonstrate that although the MIP-2 chemokine signaling is not enhanced, the copper-deficient neutrophils are stiffer (Fig. 2) and, therefore, less likely to deform and pass through the small caliber lung capillaries.
The data bolster our hypothesis that dietary copper deficiency causes proinflammatory changes in neutrophils (3). Further experimentation revealed that the reason for the loss of deformability is likely caused by greater polymerization of F-actin in the copper-deficient neutrophil (Fig. 4). Based on the results, we conclude that the excess accumulation of neutrophils in the copper deficient rat lung is the result of changes in the biomechanic-deformability properties of the neutrophil
During an acute inflammatory response, endothelial P-selectin (CD62P) can mediate the initial capture of neutrophils from the free flowing bloodstream.
adhesion of neutrophils to P-selectin in a flow chamber showed there were more adhered CuD [deficient] neutrophils than CuA ones
neutrophil migration under agarose showed that the CuD neutrophils moved farther than the CuA group in response to IL-8 but not fMLP
these results support the theory that dietary copper deficiency has proinflammatory effects on both neutrophils and the microvascular endothelium that promote neutrophil−endothelial interactions
In the current study, copper-deficient neutrophils migrated more readily through a monolayer of normal endothelial cells than did the copper-adequate neutrophils (Fig. 2). Similar increased neutrophil chemotaxis has been reported in vivo in the copper-deficient heifer
Nutritional supplementation with copper in the rat. I. Effects on adjuvant arthritis development and on some in vivo- and ex vivo-markers of blood neutrophils - Inflammation Research The nutritional copper-supplementation: 1) significantly inhibited the adjuvant-arthritis development (33% ± 5, P<0.01); 3) significantly decreased the percentage of cell adhesion by an average of 41% ± 19 (P<0.01).¶Conclusions: The copper-supplemented diet has an anti-arthritic effect which may be also primed by the effect of copper on the expression of the neutrophil cell-adhesion molecules.
2. For the budespride - Bromelain should be a good replacement.
like the corticosteroid it will skew immunity at doses over ~50mg ( budespride might not effect T cells but the neutrophil migration blocking action probably means lower immunity - as a tradeoff to lowering the neutrophil damage),
Bromelain removes surface molecules of immune cells & changes immunity. specifically reduces neutrophil migration to sites of inflammation a lot,
so bromelain will give a similar effect as the drug used at 100mg+ Bromelain treatment decreases neutrophil migration to sites of inflammation - PubMed
and is backed in ulcerative colitis orally by a case report about 2 women who gained benefit within a couple weeks of higher dose

by the photos the severe ulceration completely reversed to healthy tissueSuccessful Treatment of Pyoderma Gangrenosum with Potassium Iodide
A 35-year-old woman visited our hospital with multiple tender necrotic ulcers on her arms and legs. Laboratory examinations showed no abnormal findings except for a slight increase in C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR). A skin biopsy taken from the margin of a leg ulcer showed oedema and massive infiltration of neutrophilssurrounded by lymphocytes and histiocytes in the dermis, and necrotic epidermis with hyperplastic change. There was no evidence of vasculitis. Tissue cultures did not reveal any pathogenic microorganisms. She had neither systemic involvement nor accompanying complications such as arthritis, inflammatory bowel disease, haematological disorders or malignancy. A diagnosis of classical type idiopathic PG was made.
During the following 10 years, the ulcers constantly recurred on her extremities despite systemic treatments. This time, while continuing to take prednisolone 17.5 mg/day together with dapsone 50 mg/day and minocycline 200 mg/day as an adjuvant therapy, a well-demarcated new ulcer emerged and extended with marginal pustules following a minor injury on her left lower arm (Fig. 1a), and new lesions developed on both legs as well in 4 months. Instead of increasing the dose of steroid, we started oral KI at 900 mg/day. Surprisingly, the formation of new pustules almost stopped within a few days and improvement of the ulcers was observed accordingly (Fig. 1b and c). The dose of KI was increased to 1200 mg/day after 2 weeks, while the ulcers continued to regress.
Oxidation of I- [iodide] by the H2O2/peroxidase system leads to the formation of iodinium ions I+ which bond to thyroglobulin by electrophilic substitution. However, it is not clear whether I- is transformed directly to I+ or whether it passes through a molecular iodine intermediate
https://pubmed.ncbi.nlm.nih.gov/7104217/polymorphonuclear leukocytes [neutrophils]. Three oxygen intermediates, superoxide anion (O2-), hydrogen peroxide (H2O2), hydroxyl radical (OH.) and chemiluminescence were included in assay studies. Dose response studies were performed with therapeutic doses of the drugs (10 microM--mM). We found that both potassium iodide and dapsone significantly suppressed the generation of oxygen intermediates, except for O2
^ so by this , taking it for the 2-4 weeks needed to see results would allow repair without enough time to see the thyroid adjusting effect reverse again, after the 'thyroid escape' occurs within 2-3 days of excess iodideFortunately, with the dermatoses for which KI is currently indicated, it is likely that any therapeutic effect will be apparent within a few weeks. This is within the time frame that thyroid autoregulatory processes will ordinarily allow for escape from the WCE. If therapy with KI is continued for more than 1 month, however, a screening TSH would be prudent to ensure that iodide-induced hypothyroidism does not ensue. If iodide-induced hypothyroidism is detected, these changes are reversible by discontinuing the administration of KI. In a study of 7 patients with iodide-induced hypothyroidism, serum T4, T3, and TSH concentrations returned to normal within 1 month of iodide withdrawal.