m_arch
Member
I'm curious as to why my CP is so low, buteyko often talks about having a CP under 20 seconds as dangerous.So it seems that your metabolsim works fine in peat terms. Out of curiousity, why then do you want to improve your CP?
Well this is some new info....
according to buteyko's chart, ETCO2 and control pause should correlate with one another (this is different to what artour rakihmov says, where he has an article about how etco2 isn't a good measurement):
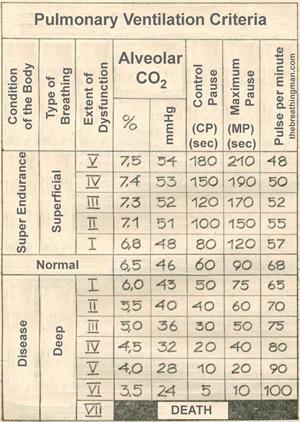
If alveolar is the same as etco% kPa (my assumption, I assume strong correlation), then I should have a 40-50 second control pause.
Well, my 'control pause' (comfortable pause time) is around 10 seconds. However I measured my maximum pause as 60 seconds today... which would correlate to 5.5% which is about right. My pulse is also around 65 and my %kPa is 5.5 to 6.0, so perhaps they are not so different and for some reason or another I just have an unusually bad ability to do a control pause.