Confirmation of Vaccine-Associated Mortality
The Chloroquine Wars Part LXXII
 roundingtheearth.substack.com
roundingtheearth.substack.com
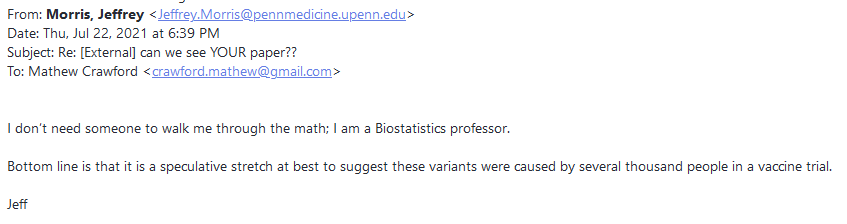
"If you cannot show me a peer-reviewed paper published in a corrupt medical journal backing your calculations of vaccine-associated mortality, I'm going to have to assume that these mafia organizations are telling the whole truth about their vaccine products without reviewing their data, and accepting the 0 in the mortality column that hasn't yet been studied." -Jeffrey Morris (paraphrasing)
To be fair, I'm not being fair. And it's not just him. It's a lot of very obtuse people who should show more responsibility from their positions. But I'm being mostly fair, and that's a lot fairer than they are.
Exhibit A: A Peer-Reviewed Paper in a Journal That Doesn't Publish Surgsiphere or Obviously Absurd Research Pushed by Powerful Interests
A new hero has emerged. Mostly-retired scientist Ronald Kostoff, PhD, and a highly experienced team, just had their paper published. The appropriate, if understated title of the paper is
Let us appreciate his restraint in never using the word "***holes" anywhere in the paper. At the age of 84, he maintains a level of polite discipline in the face of ***holes I can scarcely muster on my better days.
Kostoff worked in the past as a Georgia Tech affiliated researcher (or consultant or whatever the correct term is now), has 30 years of government service, and a long publication history that includes an amazing breadth of topics including neuropsychology, information science, research and development management, molecular mass spectrometry, citation analysis, competitive intelligence, natural language processing, naval engineering, text analysis, and now analysis of what ***holes refuse to analyze (soon to be a new category at researchgate). He published on disruptive technologies before it was cool.
Okay, okay, let's take a look at what Kostoff et al found:
Apologies to anyone who just fell out of their chair and bumped their ***hole. Read it again if you need to.A novel best-case scenario cost-benefit analysis showed very conservatively that there are five times the number of deaths attributable to each inoculation vs those attributable to COVID-19 in the most vulnerable 65+ demographic. The risk of death from COVID-19 decreases drastically as age decreases, and the longer-term effects of the inoculations on lower age groups will increase their risk-benefit ratio, perhaps substantially.
Kostoff also departs from the narrative by expressing concern over life-changing harms to young people given the much longer life expectancies and quality years they have in front of them.
Sometimes, I read a paragraph, reflect on authors with competing opinions, and ask myself, "Who do I want to trust (on a human level)?" Such a bias does not get to definite answers, of course, but I strongly suspect there is a high correlation.For example, the trials and VAERS reported clots that resulted in serious symptoms and deaths but gave no indication of the enhanced predisposition to forming serious clots in the future with a higher base of micro-clots formed because of the mRNA intervention. The latter is particularly relevant to children, who have a long future that could be seriously affected by having an increased predisposition to multiple clot-based (and other) serious diseases resulting from these inoculations.
Note for those who want to read this paper for full understanding: While you can understand the analysis in many papers on a fundamental level without reading the appendices, this paper is not one of those. Nearly the full meat of the analyses are in the appendices, which is to say that the primary text serves somewhat like an abstract. And for those worried about the background deaths rate computations, Kostoff and crew provide a short-range sensitivity analysis.
Right here. Kostoff and his team state what should be obvious to anyone who cares about an honest assessment---that there is a need to examine bodies to ascertain anything like a positive risk-benefit assessment of the vaccines. This is true both on the level of autopsies, but also on the level of seriously harmed patients whose life expectancies and quality years may now be significantly reduced. Maybe this is the moment to point out that no human even uttered the phrase "mild cases of myocarditis" prior to the CDC's recognition of the avalanche of such cases in young recipients of COVID-19 vaccines. Such heart damage is permanent, often results in dramatically shortened life spans, and can result in unpredictable sudden death at any time.In light of these data, the question may arise as to why there were no inoculant-attributed deaths in clinical testing of inoculants. The answer is that neither Pfizer nor Moderna included frail patients and included only a small number of very elderly patients - those over 75 accounted for 4.4 % of the total tested for Pfizer and 4.1 % for Moderna. While they could not in fact determine a causal relationship between inoculation and death, they also could not rule out that the inoculations had accelerated the deterioration of the condition of those patients [33].
That is to say that when either Steve Kirsch or I claim there may be 150,000 to 250,000 deaths associated with COVID-19 vaccines, we may be talking about a floor. The true number will likely expand---maybe dramatically---over the coming years. This is a truly large-scale and still ongoing human tragedy.
And while the risk-benefit analysis doesn't look good for anyone taking the vaccines, it looks absurd and frightening for children. Emphasis mine.
While Kostoff has not been contacted by The New York Times, The Washington Post, 60 Minutes, or other important media outlets, TrialSiteNews has already interviewed Kostoff. The veteran scientist also honored Steve Kirsch with a phone call today while several researchers (and this here goofball) listened in. Kostoff complimented the work of Jessica Rose, PhD (who happened to be in attendance), Kirsch, and others who carried the water on VAERS research, including contributions to Kirsch's several arguments (including some of my own) that there appear to be 150,000 to 250,000 vaccine-associated deaths just in the U.S. alone. While I won't report on what all was said in an otherwise private conversation, I can say that Kostoff sounded like a sharp-minded and active man who isn't going to kill himself and doesn't suffer ***holes in science gladly.What does this mean in the real world? In the USA, there are approximately 4,000,000 children in each age year for adolescents. Thus, there are ˜16,000,000 children in the 12–15 age band. A serious adverse event, including death, that occurred at a 1/800 rate would not be detectable with high confidence in a sample of 1005 people. Thus, the results of the trials for 1005 children would allow for 20,000 children to suffer a non-trial-detected serious adverse event, including death, when extrapolated to potential inoculation of all children in the 12–15 age group! Given that the risk of contracting COVID-19 with serious outcomes is negligible in this population, proceeding with mass inoculation of children 12–15 years old based on the trials that were conducted cannot be justified on any cost-benefit ratio findings.
Exhibit B: Because All-Cause Mortality Best Demonstrates the Immediate Point
When we have to worry that public health authorities may not be keeping all the right statistics in all the right ways, the best place to look is at a number that doesn't change when deaths might be smuggled between categories. Perhaps with this notion in mind, Risk Information Management Professor Norman Fenton set out to break down and compare all-cause mortality rates in England between vaccinated and unvaccinated populations. The results are quite interesting.
Okay, maybe we're not all going to die, but this looks pretty serious. In this first graph, it looks like the vaccines are highly effective at the outset of the vaccination campaign, but understand that during the first few weeks, those dying are largely people already sick or in poor health who wouldn't be vaccinated in such a program. By four months into the program, the vaccinated started dying at a faster rate.
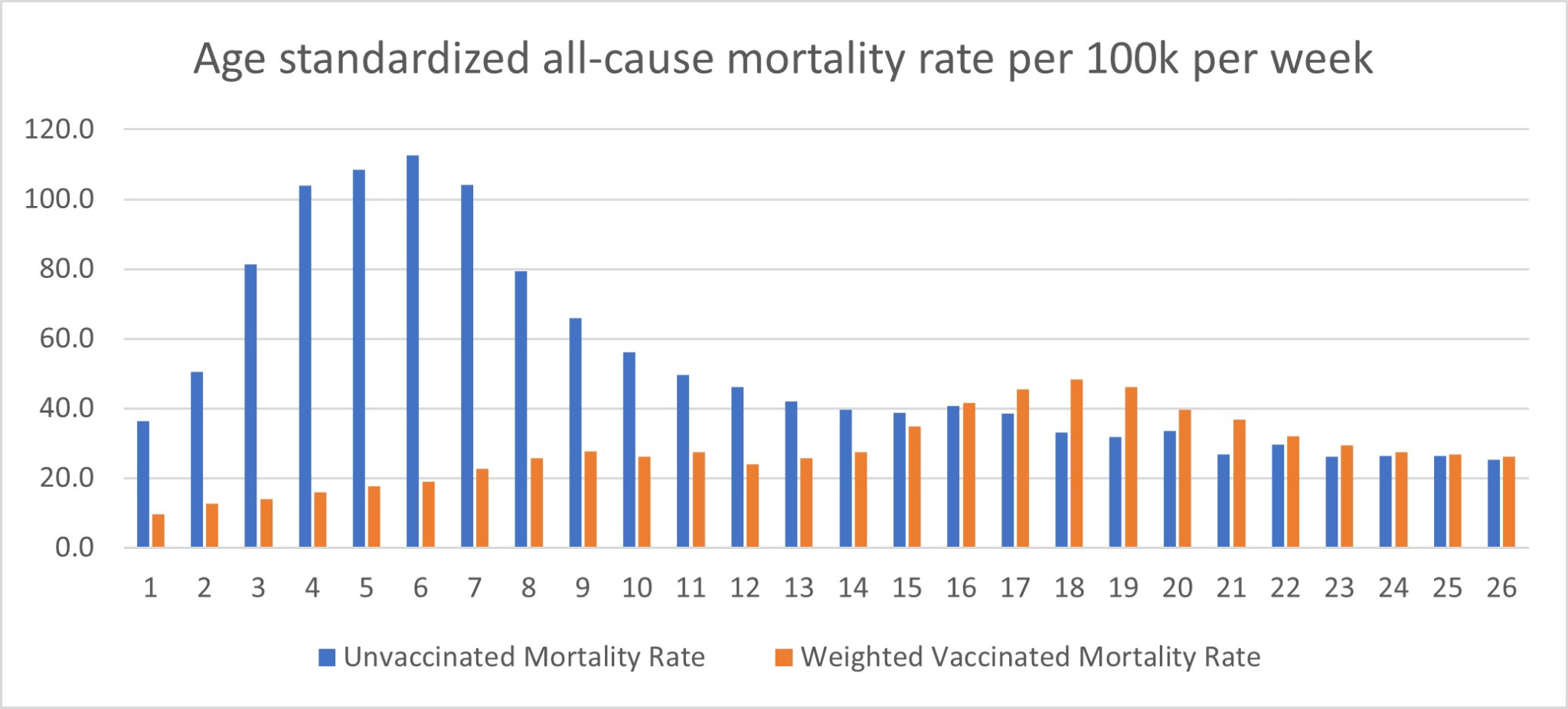
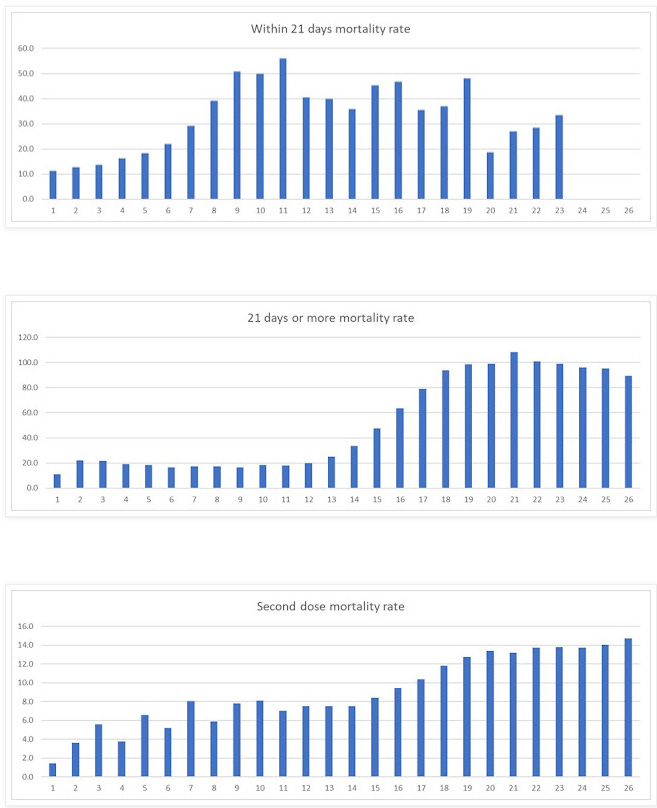
And here it appears that while mortality rates among the unvaccinated are declining over time, they seem to be increasing among the vaccinated.
This isn't going to help the make-believe case for plugging in zero deaths into a risk-benefit analysis on vaccines rather than my more reasonable approach of running a sensitivity analysis to see what happens.
Subscribe now
Exhibit C: Character Assassination Without Counter-Analysis
Jeffrey Morris's "takedown" of Steve Kirsch was obnoxiously focused away from the most important points (a handful of Jeffrey's comments could certainly be viewed as constructive criticism, otherwise, were they delivered in a more even-handed tone---Steve's first document was certainly unwieldy and some of the claims needed refining, which Steve has done and continues to do over time). Of course, Jeffrey's refusal to mention or asterisk computations he performs that depend on variable mortality numbers as if the variable is necessarily zero seems like some of the most bold statistical malpractice I've ever witnessed---even if it's governed by some sort of invisible consensus of ***holes.
Except that it's not a consensus opinion, and the problem is that authorities who should be studying the problem seem happy to ignore it while refusing to answer emails discussing it. Also, science isn't conducted by consensus, even if The Science works that way amongst gatekeepers. All science and analyses should be published with an understanding the results are still always under discussion. Heck, it's still science and it's still debatable even when it hasn't been published or peer-reviewed. Peer review and publication are just steps intended to raise the status of results through experts who are supposed to understand what they're reading, and which has been thoroughly gamed over the years to the point that even the editor of the The Lancet complains that his journal industry is captured by pharmaceutical interests (in a "It's all corrupt, but no not me" kind of way).
Instead of zero-ing in on the primary point of contention (that authorities seem to be doing more to block autopsies than to study them, while pathologists in other nations raise alarms saying that a substantial number of the examined bodies were killed through vaccination), Jeffrey poo poos concerns over the Japanese (vaccine/free spike) biodistribution report by calling the omission of proportionality at the injection site "blatantly misleading". But he skips the important step of asking the question, "Do we know enough to understand the results of this toxicity analysis---for how long the build-up in the ovaries might last, whether that could lead to fertility effects, whether outlier patients might have worse results (severe COVID-19 is itself an outlier phenomenon to begin with)?" His overly brief exploration seems only in service to saying, "We don't have proof this harms humans," when the real point should be that, "We don't have proof that this doesn't harm humans [and this is an existential issue]." At the level of basic judgment, this is a fat thumb on the scales of concern.
A Biostatistics professor whose contradiction to "lack of attention" to serious adverse events completely skates over the fact that the CDC failed to act for months after the signals of serious heart/cardio issues emerged.
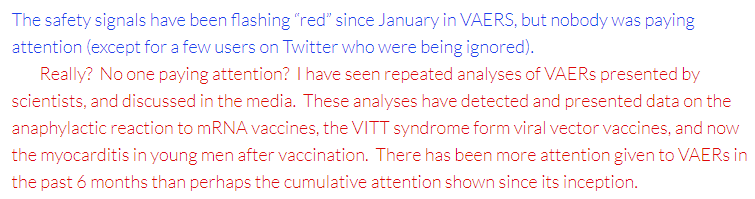
Jeffrey's response here is entirely rhetorical, and I suspect he doesn't know the history of the flags raised over the signal detections. It was weeks prior to the CDC's meeting in late June on the topic that they were made aware of the problem by staff at the University of Washington, which happened only weekly after the Israeli government broadcast the problem, which itself happened months after Robert Malone and Bill Dumouchel were discussing and getting to the bottom of the problem [in January], which is incidentally the beginning of the story of how the inventor of the mRNA vaccine technology did that thing a scientist does when they discover evidence, and changed his mind about the safety of the current application. And if you're wondering why that information had to travel from a doctor at the DoD to a data mind at Oracle to Israel to Washington state to the CDC, well, apparently Jeffrey isn't weirded out by that. I suppose it's good enough that he didn't declare it devoid of meaning prior to peer-review. Much of the rest of the "take down" is similarly rhetorical, lacking in perspective, and with no substitute analysis that would require the courage to take a position on the actual numbers, which is the piece where you'd think to find added value from a Biostatistics professor, first and foremost.
But all that's just the appetizer...
Politifact appointed veteran sports writer Tom Kertscher to "fact check" Steve Kirsch and his compilation of analyses from himself and several statisticians. Ahem. While I would like to say that Kertscher's steps into the world of serious biomedical statistics was brave, and that he must have worked hard to quickly achieve relevant expertise at the task, I'm mostly left looking for some reason not to call him an ***hole. Kertscher refused multiple offers by Steve to talk through the evidence (including new papers coming out at the time by Kostoff and Rose) in order to sort out the absurdity that is this "fact check". Kertscher's declarations seem like a zero-value-added way of saying "officials must be correct, so Kirsch pants on fire".
Edit: Kirsch's response is devastating.
This is the very essence of pseudo-science. Ibn al-Haytham is rolling over in his grave. We know that because there is no expiration on this obvious nonsense about "mild cases of myocarditis".
 Rochelle Walensky, MD, MPH @CDCDirector
Rochelle Walensky, MD, MPH @CDCDirectorTo put this into perspective, if we vaccinate 1 million 12-17 year olds, we could see 30-40 MILD cases of myocarditis. In this same 1 million, through vaccination we AVOID: 8,000 cases of COVID-19, 200 hospitalizations, 50 ICU stays & 1 death. The benefits far outweigh the risks.
Good Morning America @GMA
.@ABC NEWS EXCLUSIVE: CDC Director Dr. Rochelle Walensky weighs in on risk of myocarditis from COVID-19 vaccine. https://t.co/afVFZzWkrL https://t.co/InCcMVaC9B
June 24th 2021
1,371 Retweets3,597 Likes
I feel more than a bit of transitive offense of the "pants on fire" fact check because the phrase is obviously a dance around accusations of lying, and part of the analysis Kirsch promotes is mine---not that Kertscher wrote a single word that contests it. I'm pretty sure Kirsch will sue Kertscher for defamation, and I may join in myself on the principle that not defending your integrity is to abandon its defense. I make this substack intentionally as transparent as possible, and while I don't [yet] have a github where I'm stacking spreadsheets or code, I did send Kirsch my spreadsheets when he asked to review them, and I've shared them with a few other people capable of poking holes in the work. While they are still in "first order analysis form", I've felt that the cost of polishing them for publication was greater than the benefit of further analysis and writing, though the work may still be polished and published by other researchers. Kostoff's paper may make that a moot point.
My sincerest apologies if any ***holes were offended or degraded by extreme associations present in this article.