healthiswellth
Member
- Joined
- Feb 6, 2020
- Messages
- 71
Hi,
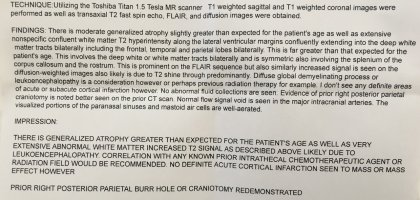
I was hoping you all could take a look at my father’s MRI and possibly recommend which products you think might help. He is receiving chemotherapy For cns lymphoma. Has diabetes (using pyrucet, magnesium, b vitamins). Has high lactic acid, low co2, high procalcitonin. My main concern is restoring his brain function.
If you could recommend products/dosage, I would really appreciate it. Also, would someone please share Dr. Peat’s email — I’m not sure how to find it and I would really appreciate his input.
Thank you
I was hoping you all could take a look at my father’s MRI and possibly recommend which products you think might help. He is receiving chemotherapy For cns lymphoma. Has diabetes (using pyrucet, magnesium, b vitamins). Has high lactic acid, low co2, high procalcitonin. My main concern is restoring his brain function.
If you could recommend products/dosage, I would really appreciate it. Also, would someone please share Dr. Peat’s email — I’m not sure how to find it and I would really appreciate his input.
Thank you