2thecloudsabove
Member
- Joined
- Apr 17, 2017
- Messages
- 106
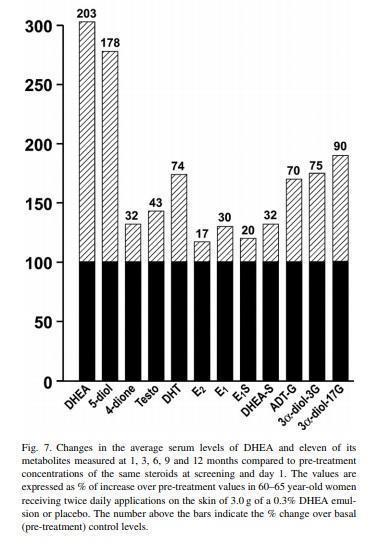
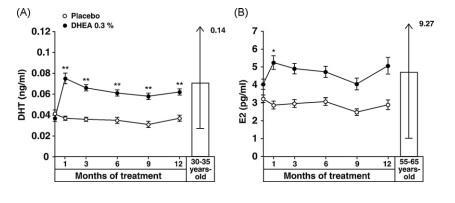
Nobody knows that as it depends on many factors, such as stress and inflammation. In higher doses it is estrogenic as evidence by increased estrone and decreased androgen levels in 35+ year olds.
Dr.Peat says we decline dhea production with age at about 2mg/decade rate after 25, so that should be the amount to be restored. So if oral administration has 3% aprox bioavailability, we should aim for (i.e. for 1 decade) 2/.03= 66mg dose? then we'd absorve the 3% equaling to the 2mg target. Is this right?